MakeBirthEasier
Make Birth Easier Campaign for mums, for babies and for midwives
Fetal Navigation Techniques: published in The Practising Midwife journal
Here is my article published in The Practising Midwife journal, December 2017 Issue – Space and Place.





The Actually Useful, Very Sensible and Practical Guide to Make Birth Easier Part 2 – Quick Guide to Make Birth Easier

Guide to Make Birth Easier – Have You Read Part 1?
– Have You Read Part 1?
Part 1 of this Guide to Make Birth Easier introduces fetal positioning, what it means for your labour – even if baby is head down – and how fetal navigation techniques can help reduce labour time, and make birth easier for you and your baby.
It also covers the benefits of birth preparation, and touches on reducing your pain levels and boosting your labour progress with your naturally produced labour hormones, a.k.a. oxytocin.
If you haven’t read it yet, you can find it here.
Below, in Part 2 of the Guide to Make Birth Easier, you can find out HOW TO…
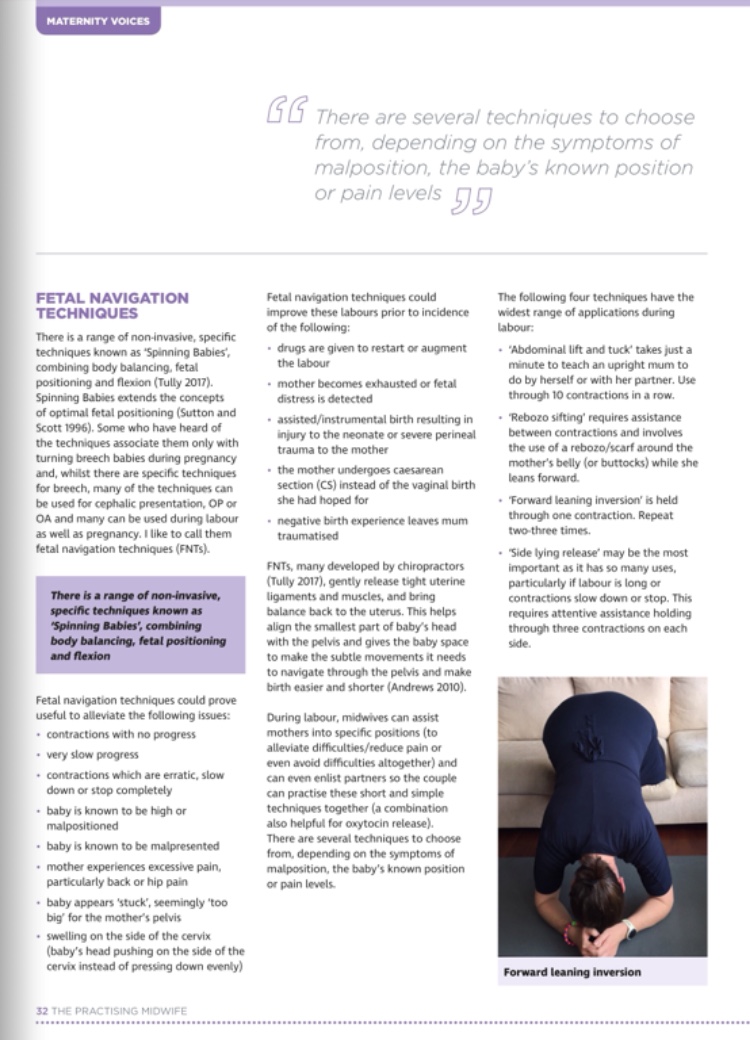
Fetal Navigation Techniques
Fetal navigation techniques are not only for turning back to back, or breech babies. Even a labour with a baby in a seemingly ideal position (HEAD DOWN and facing mummy’s back) can be overly long and difficult, or contractions can slow down or stop.
Fetal navigation techniques, gently relax and release tight ligaments and muscles, and balance the uterus, giving baby space to do the subtle movements it needs to and help align the smallest part of baby’s head with the pelvis to make birth easier and shorter.
This Guide to Make Birth Easier focuses on the 4 particular techniques which have the widest variety of uses.
A. Learn techniques 1 to 3 below (referred to as the Three Sisters of Balance on SpinningBabies.com).
B. Print out the pages and read thoroughly. Follow instructions carefully to make sure they are appropriate for you and they are done correctly for safety and to make sure they work well (some don’t do anything if not done correctly).
C. Practise during pregnancy, as per the instructions, to balance your uterine area and so that they’ll feel easy and comfortable during labour.
D. If you are right at the end of your pregnancy it is not too late as you can use them right up to the start of labour and during labour itself.
E. USE THESE TECHNIQUES DURING LABOUR for:
- contractions with no progress (contractions not getting closer together, stronger or longer),
- slow progress,
- contractions which slow down or stop completely (stall),
- if you know your baby is in a less than ideal position, or,
- if you have hip or back pain, or you have swelling on your cervix (baby’s head may be pointing towards your hip or back or onto the side of the cervix instead of straight down through the pelvis).
- Technique 4 shown below is for labour only as it needs contractions to work (even if they’re irregular) so wait until labour starts to use this one.
- REMEMBER TO TAKE THE INSTRUCTIONS WITH YOU during labour, whether that is on paper, or via your phone, tablet or laptop (remember you may not be allowed to plug in electrical devices at the hospital and there may be poor internet signal).My input is not intended, and should not be taken, as constituting medical advice. Before you attempt any of the SpinningBabies.com or other fetal navigation techniques I’d advise you first to print out the pages ‘Rebozo’, ‘Forward Leaning Inversion’, ‘Side Lying Release’ and ‘Abdominal Lift and Tuck’ and show a copy to your doctor or midwife for discussion, where you should ask if there is any medical reason you couldn’t try any of the suggestions on those pages. As an example, for high or very low blood pressure or risk of a stroke, it is advised not to do inversions. If you have a low risk pregnancy with no contraindications, most of the techniques are usually fine. Just check first. Obviously go with your intuition and only undertake activities you feel comfortable with. You know your body and your pregnancy.
- I would love to provide you with a printer friendly version of this guide, but I prefer that you go via the SpinningBabies.com website for the most up to date version of the instructions at the time of your pregnancy/labour, as they do update their website from time to time.
- REBOZO MANTEADA SIFTING
A great technique with many uses. Helps to release tight ligaments and muscles so baby has more freedom to rotate into a better position and engage. I would also do this one before any of the others to help them be even more effective.
Click here for SpinningBabies.com Rebozo Manteada Sifting.
Click below for a video of Rebozo Manteada Sifting and Shake the Apple Tree, a relaxing alternative to sifting.

2. FORWARD LEANING INVERSION
Helps to give your uterus balance so baby can align well with your pelvis, and gives baby space to do the movements it needs to before and during labour. This technique can be done throughout pregnancy – even preconception. I used this during both of my pregnancies. Some of the photos in the link show this technique being done from stairs or a high level but I only used this off a low level sofa. Go with what feels comfortable to you.
Click here for SpinningBabies.com Forward Leaning Inversion.
Click below for YouTube clip of Forward Leaning Inversion.
Please note that although you cannot see clearly in this video clip of the Forward Leaning Inversion, the head should be hanging freely, not touching the floor or your hands (with chin tucked into your chest like you want your baby to do). Also the belly should be hanging freely and not touching the couch. After the inversion, go directly back up to the high kneeling position for 2 to 3 breaths before sitting back onto your feet for one more breath. Then bring your legs around together to the front – with knees together, and feet together to avoid pulling your pubis symphysis, before getting up slowly.
- SIDE LYING RELEASE
In my mind this technique is the most important one to learn as it has so many uses, particularly if labour is taking a long time or if contractions slow down or stop. Unfortunately this is also the one that doesn’t work at all if not done correctly so do pay attention to the details and do take the time communicating with your helper to adjust your position and get it right for maximum benefit. Practising this during pregnancy will help you feel more comfortable doing it during labour as it feels rather unsteady at first (if it doesn’t feel unsteady you’re doing it wrong!). I used this during my first labour after doing the rebozo, and my labour changed dramatically within minutes. Do it on BOTH SIDES.
Click here for SpinningBabies.com Side Lying Release.
Click here for YouTube clip of Side Lying Release.
A note here on pelvic floor muscle exercises (kegels) – some people wonder about the effects of using this technique when they have been doing kegels to strengthen the pelvic floor. This technique only lasts for a few hours (it’s effect is temporary) and helps the muscles be balanced and supple enough for baby to pass through more easily. Please do continue with kegels during pregnancy to give the pelvic floor muscles good strength and muscle tone so they are strong enough to help baby make those all important rotations.
- ABDOMINAL LIFT (AND TUCK)
This is the best technique for turning a ‘back to back’ baby (baby facing your tummy) and also for helping a high baby come down and engage in your pelvis. Also if baby is stuck on the brim (top edge) of the pelvis this is good for helping baby move into the pelvis. Indicators for a back to back baby can include irregular or stop/start contractions. I used this technique in the early stage of my second labour to turn my back to back baby in an hour and regulate my own contractions so that I could cancel my induction appointment!
If previous labours have been fast – only do this if you have your care provider nearby.
Click here for SpinningBabies.com Abdominal Lift and Tuck.
I reiterate that techniques 1,2, and 3 can be done during pregnancy AND labour, and technique 4 is for labour only as it needs contractions to work.
Medical terminology
For clarification I’ve given a few translations for some of the medical terminology from SpinningBabies.com below. For further explanation you could contact a medical professional. SpinningBabies.com is written by a midwife for other midwives so the language can be quite medical.

Abdominal fascia: abdominal tissues.
Oxytocin: a naturally produced hormone essential to labour progress, and important for bonding with baby and milk production.
Pitocin or Syntocinon: induction drugs (synthetic oxytocin) used to induce labour or strengthen labour contractions during childbirth, and to control bleeding after childbirth. Synthetic oxytocin does not behave in the same ways as the naturally produced hormone.
Crown: the smallest diameter of the head.
Flexion: the degree to which baby’s chin is tucked in to the chest (tucked in is best)
Asynclitic head: head is presenting first and is tilted towards the shoulder.
Posterior/Occiput Posterior (OP): back to back baby (occiput = back of the head, posterior = back).
Anterior/Occiput Anterior (OA): baby facing mother’s spine (occiput = back of the head, anterior = front).
Left Occiput Anterior (LOA): baby facing between the mother’s right hip and her spine with its back on the mother’s left side (occiput = back of the head, anterior = front). Other variations are ROA and so on.
Breech baby: baby with head up and bum or feet down.
Transverse baby: baby lying sideways with head on one side and bottom and feet on the other.
Oblique baby: baby in a diagonal lie with head in mum’s hip.
Antenatal or Prenatal care: care while you are pregnant.
Contraindication: medical reason not to do something.
Malposition: head down but not in an ideal position.
Malpresentation: crown of the head is not down first i.e. another part of the body is presenting at the cervix such as feet or bottom (breech), side (transverse), shoulder (oblique), or forehead/face (brow presentation).
First stage: the neck of the womb (cervix) gradually opens up to 10cm. Described in two phases (latent and active or established labour).
Latent phase: early labour.
Active/established phase: contractions are regular, every five minutes and lasting for at least a minute.
Second stage: baby descends through birth canal and out of the vagina – transition from 1st to 2nd stage is at full dilation (10cm).
Third stage: delivering the placenta or afterbirth.
Transition: cervix reaches maximum dilation of 10cm and baby starts descending.
Gravity, Movement and Balance are your friends. Let them help you.
Now you know how to set yourself up for easier birth, here are some helpful hints and tips to manage the rest of your labour.
Stay Off Your Back – Let Gravity Help
Lying flat on your back makes labour/birth more difficult for you and your baby in many ways – so STAY OFF YOUR BACK.
Being on your back is a position which makes things easier for the birth attendants (better view), not for you or your baby and certainly not for labour.

Being upright, walking, crouching, being on your knees leaning forward on your arms/bed/couch/birth ball – all help labour be shorter and easier. Move around.
If you are tired, you can hang on to your birth partner or lie on your side. Left side is the best lying down position if you are going to spend much time in one position – either side is fine if you move around periodically. Avoid staying on your back for long if at all. Try to change positions fairly regularly.
Even if they want to strap on the monitors, or put in an IV you could stand to go to the toilet, so it is possible to be upright and monitored even if the upright part is for short periods of time. You do have the right to stand up if you want to, or sit on a birth ball (exercise ball) or turn around and kneel or lean on the bed. Be more active – even if it’s not super comfortable at first, it will be of benefit to your labour and is likely to reduce pain. Use your instincts and find positions that work for you.
If for any reason you cannot stand up then LIE ON YOUR SIDE. Even with epidural you can be on your side and midwives can help you to change positions periodically even if some positions are just moving your legs as this changes the angle of your pelvis. Ask them to help you move.
If you do have epidural or other limited mobility, a great way to aid labour progress is to use a peanut ball. Unfortunately only a few NHS units currently have these available to use. It has been suggested that if a woman knows in advance that she will be having an epidural, she could consider getting her own to take into hospital with her.
Click here for a great blog post from scienceandsensibility.org describing peanut balls.
Some generally helpful positions in labour, even with monitors on, are shown at betterbirths.rcm.org.uk. Click here to view.
Move Your Pelvis
Bending your knees, squatting, rotating on an exercise ball, doing pelvic tilts, lifting one foot up/putting one foot on something low or high (depending on your comfort), walking up stairs sideways – all help to open your pelvis and let baby through more easily. The pelvis is not a straight tunnel and your movement lengthens and shortens the passageway quite considerably so moving around really does help your baby navigate down and out.
A wonderful way to get your pelvis moving is to dance. Yes, I did said dance! Rotating your hips in a figure of eight shape or belly dancing are fantastic for helping your baby come down. This is also a great way to relax a little more and you can do it alone or with your partner for support and added oxytocin releasing closeness. If you need sturdier support you could lean against a wall or a chair. Maybe put some music on!

These movements can have a positive effect on baby’s position during pregnancy as well as during labour so get going now!
Labour Hormones = Labour Progress
Hold onto your birthing partner. Closeness helps your labour progress well because it helps you release the crucial birthing hormone oxytocin. Your birthing partner doesn’t need to be male.
Even being around other sympathetic women can help you release oxytocin so having a female friend or relative, or an independent midwife (http://www.imuk.org.uk/) or doula (https://doula.org.uk/), there for you as a trusted advocate, to help you relax and communicate with your care providers can be of great help to you and your labour.
A constant presence can feel particularly supportive to you on a busy labour ward where midwives may be very busy or changing shifts and unable to stay with you throughout your time there.
To find out more about oxytocin and the effects on your labour of having it and of not having it, see Part 1 of this Guide to Make Birth Easier here. Hugs all round!

Avoid Paracetamol
Research shows that paracetamol can make your labour much longer because it inhibits the release of prostaglandins which have hormone like effects that your labour needs to progress properly.
Many midwives are not yet aware of the new research available on this, and so they are often telling mums in early labour to take a couple of paracetamol for the pain.
Avoid paracetamol in late pregnancy and during labour. If you want to learn more about paracetamol in labour click here.
Early Labour
Early labour may not be as you expect.
Care providers usually advise that you stay at home for as long as possible unless there is some medical reason you should come in early. This is because home is more comfortable and quiet which helps you to release more oxytocin and so helps your labour progress.
If you are feeling anxious because things aren’t happening as you thought they would – call your care providers for advice. A five minute phone call may be preferable to travelling to hospital and being sent home again.
I expected contractions to happen every 20 minutes or so and get closer together and longer in length. Instead, at the start of my first labour, I had painful contractions very close together which were long but not long enough. I didn’t know what was happening or why which made me tense and made things more painful. I phoned the labour midwives for some advice. They told me this was quite normal in early labour and to go and have a warm shower and go to bed. I thought they were crazy (“how am I supposed to sleep like this?!”) until I did it and wow did it work. The warm shower reduced the pain and calmed my contractions so much I actually got some sleep! Relaxation!

Early labour the second time for me lasted for a week, with very irregular contractions (not painful) which started and stopped again and again because my baby was back to back.
Take Opportunities
You don’t know when you will have your next opportunity, so make sure someone reminds you to:
- eat and drink small amounts regularly to help keep your energy up because you do need the energy,
- sleep whenever you can,
- go to the toilet when you can.
Relaxation Techniques
The more anxious or tense you are, the more pain you feel. Refer back to Part 1 of this Guide to Make Birth Easier to find out why.
Relaxing your mind and body literally (and immediately) reduces pain and allows labour to progress.
It’s not hippy stuff – it’s biology.
Deep breathing (lots of focus on this – see the section below on breathing techniques), warm showers, warm bath, cuddles/closeness with your partner: all these things help to relax your body and help you release the necessary labour hormones (oxytocin and painkilling endorphins) into your body, helping make birth easier, less painful and shorter.
I am well known by family and friends for being VERY easily stressed, so if I can RELAX, YOU can too. Here’s how…
If you have previously practised any meditation this is extremely useful to use during labour. See Part 1 of this Guide to Make Birth Easier to learn a bit about Hypnobirthing which I used to maintain my calm. See also the section below on breathing techniques.
Light Touch Massage, is quite strangely effective. Your partner runs their fingers gently across your back, arms, neck etc. Click here for a clip showing how to use light touch massage. This a proven pain reducing technique, not just for labour either. I found it very helpful during my second labour and wished I had tried it during my first. Have a practise with your partner in advance so they can get used to how you like it. Again everyone is different and this type of massage can be really annoying if it’s not done the way you like it. You may also find that during labour you have changed your mind about how and where you like it, so COMMUNICATE this gently (yes gently!) to your partner in order to maintain your calm.
Laughing is also a brilliant way to relax your mind and your body. No I’m not kidding, it is allowed to laugh during labour!

I mention earlier in this Guide that rotating your hips like a belly dancer helps baby’s progress through the pelvis. Well if you dance around with your partner you may find you’re relaxing more, laughing, moving and releasing those essential labour hormones all in one go!
Water in labour is fantastic for relaxation and reducing pain levels. I really felt the difference in early labour in the shower and later at the end of labour when I got into the birthing pool. I entered the pool towards the end when things got very intense. Some people like to get in and out more than once. You may find getting in very early in labour isn’t as powerful as later on but everyone is different so if you want to get in early, go ahead.
Small note here – if you are using a TENS machine (also helpful for a time) – remember to turn it off before trying to remove it or your fingers will get zapped… Yes ok, not the brightest move (especially while climbing into the pool) but in my defence I was a bit distracted! At least it made us all laugh at the time!
Imagine your body opening up and letting your baby out. Visualisation can be a very powerful tool if you give it a chance. Your body is designed to open up. Trust that it can and it will.
I have listed several relaxation techniques here – basically find something that works for you in each stage of labour and use it, whatever it is. If you have something else that you find helps you relax, so use that. Remember to have something fairly powerful up your sleeve for active labour and transition to keep you calm, focused and internalised as labour is surprisingly intense.
Breathing techniques
Breathing techniques – you may be thinking “yeah whatever” – but seriously they work!
Click here for a clip showing how to do the Hypnobirthing breathing techniques 4 in / 8 out, 20 in / 20 out, and J Breathing.
CALM BREATH 4 in / 8 out
I practiced the 4 in / 8 out technique when I went to bed and it helped me to sleep throughout pregnancy when other mums-to-be were struggling. Because I practiced it every night, it came naturally and easily during labour. I use this technique even now, years later to help me to get to sleep when I need it.
This technique is for throughout early labour and between contractions during active/established labour.
SURGE BREATH 20 in / 20 out
During the active/established phase of labour, when contractions are much more intense, I used the long, slow breathing technique during contractions (surges) where I tried to count to 20 on the in breath (while blowing my tummy up like a balloon) and then 20 on the out breath (releasing my tummy). This is pretty difficult to do – it’s supposed to be. The concentration and effort you need to achieve this is key in relaxing you as you are focused more on your breathing than on yourself. Focusing on more than two things at the same time leaves no room in your head for thoughts, worries, fears. It’s distraction, and it works. You may prefer to count to ten very slowly rather than getting frustrated trying to count fast through the teens to 20. Stick with it and have your birth partner supporting you by keeping an eye on you and regularly reminding you to breath, count and move your tummy – this will make a big difference to your pain levels, works with the movement of your contractions and keeps oxygenated blood flowing to your uterus.
J BREATH Pushing
Click here for a little background information in the section ‘No Purple Pushing Please’ in Part 1 of this Guide.
J Breathing is a directed breathing technique to help you avoid tiring yourself out. Apply pressure using your uterus not your whole body. Use only your abdomen/belly/groin to push – as if you are trying to poo – sorry for being so graphic but it’s true. You would not tense your whole body to poo – you’d only use your poo muscles!
Focus on/visualise three things at the same time – long slow breaths; the top of your uterus pushing baby down and; widening your birth canal for baby to come through. The J Breath is a big breath in, and then the out breath is directed down and outwards like a J shape. This is something you can practice during pregnancy while you’re sitting on the toilet. Follow your instincts when it comes to how strong your pushing is. You may find yourself pushing or just breathing baby down. Go with what your body is telling you.
NORMAL BREATHING
Use normal breathing whenever you are comfortable to do so.
If you get mixed up which type of breath to use, just go with your intuition and what feels comfortable. Whatever keeps you calm. Avoid the breathing being a source of frustration but use it as a source of relaxation – go with what works for you. Direct the breath however you feel it is helping you.
Using any of your breathing techniques, include putting your tongue against the roof of your mouth just behind the teeth. This relaxes your jaw. Weirdly, relaxing your jaw actually helps to relax your vaginal area and it is something I used during my labours! Your body is so connected inside! I had it on my reminders list for my birthing partner to remind me to do this.
ALWAYS WHEN BREATHING
Whatever kind of breathing you do, and whenever you’re doing it, whether it is during labour, or your normal daily life (this one is for your whole family too!), ALWAYS keep your shoulders and chest down and breath into your abdomen. If you watch your pet breathing, their shoulders and chest are not rising. It’s their stomach/abdomen that moves right? Humans with our daily societal stresses, start breath in stress mode sometimes from childhood. Breathing into your shoulders and chest actually activates your stress response in your nervous system so it’s best avoided if you’re aware of it. Breathing into your abdomen activates your rest and relaxation mode. You can actually control your own stress levels! Yay!
Practice every day and night so that your body becomes accustomed to breathing the right way and it becomes natural and easy. Again…relax your face and your jaw. These are such very simple tricks which have a powerful effect on your body.

Vaginal Examination – Necessary or Not?
You can politely say no thanks to vaginal examinations (VE). It is routine for midwives to do them but they do not help your labour progress. They can introduce infection (particularly if your waters have broken) and can increase pain and anxiety, which can slow down your contractions. A VE may be appropriate if there is some kind of complication and baby’s position needs to be assessed.
I only ever had one VE during each of my two labours, which was done when I first met with my midwife. Just one. You can ask the midwives/doctors kindly to keep VEs to a minimum so that you can remain more calm and relaxed and help your body progress naturally.
Medical Intervention
In some cases, medical intervention is absolutely necessary. Sometimes it may not be.
If the doctors/midwives talk about inducing you; ‘speeding things up’ by breaking the waters or giving drugs; having instrumental delivery (ventouse / forceps); or having a csection – ask if there is a medical reason for this.
You can ask if it is safe to take a little more time while you try some of the fetal navigation techniques like 1 and 3 above or 1 and 4 depending on the issue, or simply change position. You can ask what would happen if you just wait. Many times, using fetal navigation techniques to help baby adjust its own alignment can reduce labour time by hours and avoid any need for medical intervention.
Here are some questions you can ask to help you make a more informed choice:
- B What are the BENEFITS of this course of action?
- R What are the RISKS?
- A Are there any ALTERNATIVES?
- I What are the IMPLICATIONS? Will it make further INTERVENTIONS more likely?
- N What if we do NOTHING and wait for an hour or two before making any decisions?
Previous Cesarean Birth – Vaginal Birth After Cesarean (VBAC) is not a reason in itself for csection. Talk to sympathetic care providers about what the risks are for both options, specifically for your body and your current pregnancy.
BIG Baby – If they say baby is big, remember that petite women birth large babies naturally and safely every day. It is not a reason in itself for medical intervention. Many times delays in labour are due to baby not being in the best alignment with the pelvis (head being tilted a little to the side, chin not being tucked in to the chest, or very tight pelvic floor muscles can add hours to your labour and give the impression that baby is stuck). It is also not certain that your baby will be big. Ultrasounds are notoriously unreliable for determining the birth weight of babies. Baby being too big for the pelvis is actually fairly rare and associated with previous pelvic injury or severe malnutrition. There is a very in depth article explaining the research on intervention associated with big babies which I will not put the link to here, but if you would like to read it I will be happy to send you the details – please do contact me.
Learn about the options available to you so that you can make a fully informed decision, understanding the risks of one option over another. Every woman and family is different and every pregnancy and labour is different, so choices can vary considerably. It is your body, your baby. Decide what feels right for you. This may or may not be intervention.
If you are induced, or you have epidural, you will likely have constant monitoring and an IV drip. You could nevertheless have a smooth labour and avoid further intervention by using the techniques and tips in this Guide. Ask your care providers to help you change position, move around and feel safe and calm.
If you or your baby are not in any medical danger then you are within your rights to politely say no thanks to medical intervention.
Of course if you or your baby are in any danger then please follow your care provider’s advice!
Birth Plan for Vaginal AND Cesarean Birth
Write a birth plan (or birth preferences as I prefer to call it). Even if this is only so that you have investigated and you understand the different options available, medical or otherwise.
I wrote a short birth preferences list, not only for a vaginal birth, but also for a csection birth, just in case I needed one. This can make things a little more comfortable for you and also can make birth easier for your baby even after the birth.
Part 3 of this Guide to Make Birth Easier is coming soon and explains how to write Birth Preferences, including some incredibly simple things you can do that make birth easier for your baby:
- Optimal Cord Clamping (OCC) – also known as Delayed Cord Clamping (DCC) – one third of your baby’s blood volume remains in the placenta and cord at birth, so delay cutting the umbilical cord for a few minutes to allow your baby to receive all of its own blood, helping it be a stronger newborn Read my blog post on OCC here,
- Skin to Skin contact (so many proven benefits I haven’t got the space to summarise here),
- and even the new procedure for csection births, ‘Seeding the Microbiome‘ – helping to protect your baby against many diseases for the duration of its life.
Speedy Recovery
My midwife recommended I put a couple of drops of tea tree oil (essential oil) on my maternity pads post birth (heavy flow night pads are much more comfortable than maternity pads by the way). This helps to fight off infection while you heal, particularly if you’ve had any stitches.
I bought some arnica 30c Pillules (teeny tiny tablets) from the pharmacy which is a homeopathic remedy for reducing swelling, so this is great if you feel bruised or if you’ve had any stitches (perineum or csection).
*Note: Always consult your doctor, midwife or other qualified healthcare provider regarding taking any medication, homeopathic or herbal remedies during pregnancy or breastfeeding. Benefits of homeopathic or herbal remedies may be anecdotal rather than evidence based.
Recover Your Tummy – Yes It’s Possible!
One other thing I was VERY grateful for was a tip I had from a midwife within a day or two of giving birth. This was to roll onto my side and push up sideways to get up from a lying down position.
The abdominals separate down the vertical centre-line of the tummy to allow space for your baby to grow. After giving birth, these muscles are naturally supposed to knit back together again down the middle. Many women find that no matter how much exercise they do on their abdomen, it never recovers its former shape. This is because there is a gap between the two sides of the abdominals, and the name for this is ‘diastasis recti’. The gap can sometimes be small (measured by a finger or few) and sometimes it is really wide so your tummy has no support or shape (being asked when you’re due, two years after giving birth, is no fun).

The cause can often be that there was too much pressure put on those abdominal muscles too early following birth simply by sitting straight up forwards in a sit-up motion. Sitting up forwards literally pulls the two sides of the ‘rectus abdominis’ muscles apart instead of letting them knit back together. From lying down, if you roll over onto your side and use your arms to push you up sideways for a few weeks, you will give your abs time to grow together and strengthen again. I’ve wondered time and time again, why more women aren’t told about this simple thing (it drives me nuts that this information isn’t common knowledge). So, there you go!
For a few months after the birth of your baby, and certainly until your diastasis recti has healed properly, it’s best to avoid any sit ups (including the twisting kind) and planking. Just avoiding these exercises will go a long way to helping you in the first place.
There are other exercises you can use which to restore tone and shape to your abs. After my kids a few years ago, I would simply do standing crunches: standing feet hip width apart, curling my tailbone under, pulling my navel towards my spine, tensing my abs and my pelvic floor muscles (kegels), all while gently pressing my sides towards my navel with my hands. Sounds like a lot but you get the hang of it fairly quickly.
More recently I found this diastasis recti abdominal repair workout which seems to have some great reviews of success. Bonus! (Please let me know if this works for you or if you have any problems!)
You will probably want to first check if you actually have diastasis recti, and the extent to which you have it (width and depth) so that you can track your healing progress. Here’s how.
I would say take it step by step. You may want to spend a few days just doing the pelvic tilts at the beginning of the above diastasis recti abdominal repair workout video, to just reconnect with your abdominals. Once you’re comfortable with the pelvic tilts, then move on and include some of the other exercises in that video. When you’ve spent some time doing the beginning and middle sections of the video and feel stronger, add the last couple of exercises into your regular routine.
Again, please obtain the all clear from your doctor before doing any post partum exercises.
A reminder here on pelvic floor muscle exercises (kegels) – some people worry that doing the Side Lying Release (SLR) technique can relax the pelvic floor when they have been doing kegels to strengthen these muscles. It’s ok because the SLR acts for just a few hours and helps the muscles be balanced and supple enough for baby to pass through more easily. Please do continue with kegels during pregnancy to give the pelvic floor good strength and muscle tone so they are strong enough to help baby make those all important rotations.
Coming Soon:
Part 3 – Birth Preferences
- How to write your own birth preferences for vaginal birth, and
- How to write your own birth preferences for surgical birth for a ‘gentle caesarean section’.
So watch this space.
Congratulations on your pregnancy, good luck with it all and I hope even some of this is helpful to you. I used pretty much all of it!
Please do feel free to contact me if you have any comments or questions. I am happy to help!
Blog written by Alix Fernando
https://www.facebook.com/MakeBirthEasier
#MakeBirthEasierCampaignUK
The content of this blog is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.
The Actually Useful, Very Sensible and Practical Guide to Make Birth Easier Part 1 – Introduction

Make Birth Easier? Really?
Some people believe there’s not much you can really ‘do’ to make birth easier, shorter or safer.
I am not one of those people anymore.
For some women, medical intervention really is necessary, and I am all for intervention when it’s needed – it absolutely saves lives. Some women really want it – so let them have it. I just didn’t want any intervention if I could help it. Daft as it may sound to some, I was actually more scared of medical intervention than of the labour itself.
I was so terrified of labour in general (the most ‘natural’ thing that a woman can ever do?) that I realised I had to do something about it – this fear I had, I knew, wasn’t going to help me. Being an engineer, I needed to find a solution. What was it that was going to help me get through this?
So began my epic research journey into the world of labour and birth, and I have found not just one but many, super helpful things that really do (no matter how weird or basic some of them may sound) make birth easier.
I am a great believer in sharing useful information so I’ve listed my favourite techniques and tips in this three Part Guide to Make Birth Easier. I’ve tried to stick to plain English and I’ve given some explanations/translations where I couldn’t avoid using medical language, as not all of us are medically trained.
The Guide to Make Birth Easier is NOT only for vaginal birth. If you do have intervention or even a planned caesarean section, there are some tips to help you and your baby in Part 2 and Part 3 of The Guide.
Please remember that this guide is written for birth in the UK, BUT I am sure there will be things that any mum anywhere in the world could use or find useful.
Nature Works – Oxytocin
I do believe that for many women intervention is suggested far too early, when, as I have discovered, many labours need no help whatsoever apart from being left a little longer (stop rushing nature!) or given a little more peace and quiet (why do you think other mammals go and find a safe, comfortable, quiet, and often dimly lit space to birth?) and a little love thrown in. Closeness or support from a birth companion, relative or friend (this could include a doula or familiar midwife) can help a woman release oxytocin.
Oxytocin is a naturally produced hormone essential to labour progress (effective contractions), and is also important for bonding with baby and milk production. As a response to the production of oxytocin during labour, the body releases particular endorphins (another type of hormone) which act as painkillers sometimes described as similar to morphine or pethidine.
Yes you read that right – more oxytocin means better labour progress and less pain. FACT.
Oxytocin reduces if mum is anxious or tense, because, fear in the body releases adrenaline which stops the production of oxytocin during labour.
Tension can rise if mum has to move locations or if her birth environment is not private or calm (for example bright lights or extra people coming in and out of the room). This can cause contractions to slow down or even stop, which can in turn lead to the suggestion of medical induction.
Induction drugs such as Pitocin or Syntocinon are synthetic (artificial) oxytocin which are used to induce or strengthen labour contractions, and to control bleeding after birth. Synthetic oxytocin does not behave in the same ways as the naturally produced hormone and it actually inhibits or stops the production of natural oxytocin in the body during labour. While plenty of vaginal births do happen with women who have been induced, induction is a medical intervention, which can often lead to other interventions if contractions become too strong for the baby or placenta.
Contractions during induction can be longer and stronger, without a rest between them. This can be more painful for mum (leading to epidural) and cause fetal distress/reduced oxygen to the baby (leading to csection). Synthetic oxytocin does not cross the blood – brain barrier so you won’t release the painkilling endorphins as you would with natural oxytocin production. This is another reason contractions can become more painful for mum during induction. Add to this that induction drugs are usually given by IV drip and you are required to have constant monitoring, so you may be told you are confined to bed and not able to move around freely (you could ask anyway).
Many inductions are carried out to speed things up for convenience (often for care providers, sometimes for mums) and often not for medical reasons. If you’d rather avoid any intervention, you could ask your care providers if there are medical reasons that they have suggested doing it, and if not, could you wait for labour to take its course naturally. Again, cuddles with your partner, and a more relaxed, quiet and dimly lit environment help you to release more of your own oxytocin.
If labour progress does need assistance, wouldn’t it be nice if you could try some alternatives before heading down the medical intervention route? Fast acting alternatives which really work?
What Does Fetal Positioning Mean?

Have you spent time slouching at desks, driving, carrying a bag on one shoulder, or crossing your legs over your lifetime? Yup – me too. Most of us have. Our original mammal design doesn’t account for this type of body behaviour. These repeated unnatural body positions – or even a sudden stop in an accident or during sport – create imbalances in the uterus and surrounding ligaments and muscles. This reduces space in the pelvis and baby’s alignment is affected. Some babies may even turn sideways, back to back or head up due to the imbalance in the uterus. It reminds me of trying to get comfy on a long haul flight actually!

Alignment is something so simple which can in many cases be so easily and gently remedied by mummy rebalancing her uterine area, returning the uterus to the way nature originally designed it and helping baby reposition itself for easier birth – fetal positioning.
Fetal positioning, or fetal navigation techniques are specific techniques which are not only for turning posterior (head down but facing mother’s abdomen, known as back to back) or breech (head up) babies. Or transverse (sideways) or oblique (diagonal) babies for that matter. These techniques can also assist a baby in the seemingly ‘ideal’ position for birth i.e. head down and facing mummy’s spine. Even for babies in this position, labour can be overly long or contractions can slow down or stop. This can often be due to something as simple as baby’s head being tilted to the side slightly, the chin not being flexed (tucked in to the chest), or ligaments/muscles being too tight for baby to fit through. These things slow down progress and can make labour unnecessarily long and difficult. Square peg, round hole. Pretty logical.
I have to mention here that even though many malpresented babies (crown of the head is not down first) are sent directly for csection, this is because csection has been used so commonly in these cases, that many care providers these days no longer have the experience of delivering them vaginally. However, there are care providers out there who are experienced and willing to deliver these babies. If you do want to birth your breech baby vaginally, you may be lucky enough to track down a care provider willing and able to help you.
So a little further explanation on the perceived ideal or so called optimal position…As mentioned above, this is for baby to be head down and facing the mother’s back (often with its back towards the mother’s left side – LOA – see the medical terminology I have outlined in Part 2 of this Guide), with baby’s chin tucked in nicely to the chest and the crown (the smallest part of the head) aiming through the pelvis. For malpositioned babies (head down but not in an ideal position), usually time is given for a woman to labour and see if baby will rotate. In many cases this doesn’t work and after a long labour a csection is suggested. Despite this, some women have a pelvis shape that lends itself easily to back to back or breech position anyway. So, if you do labour with a back to back or breech baby, it may be absolutely fine.
Fetal navigation techniques, several of which were developed by chiropractors, gently relax and release tight ligaments and muscles, and balance the uterus, giving baby space to do the subtle movements it needs to and help align the smallest part of baby’s head with the pelvis so that baby’s route into the outside world is as easy and short as possible. The techniques can be fast acting, which is what happened to me in both my labours.
Part 2 of my Guide to Make Birth Easier focuses on the four fetal navigation techniques which have the widest variety of uses.
I practised the techniques during pregnancy so that they felt easy and comfortable during labour, which is when I used them with greatest effect. These techniques can be used during labour for:
- contractions with no progress,
- slow progress,
- contractions which slow down or stop completely,
- if you know your baby is in a less than ideal position, or,
- if you have hip or back pain, or you have swelling on your cervix.
You Can Change Your Labour
Some people may be, but I am not, Superwoman. I do not (very definitely do not) have a high pain threshold (at all! I’m a total wimp!) and I wasn’t just ‘lucky’. I worked hard at achieving my easier births because I kind of felt like I had to take action for my own sanity. I believed in the things I’d learnt and I trusted in the knowledge that my body really is designed to give birth (we are mammals after all). I was amazed by the results, as were many midwives and doctors I recounted my birth stories to.
I tend not to use the terms ‘normal’ or ‘natural’ birth, as birth is birth whichever way you do it, but, this quote comes from the Royal College of Midwives Normal Birth Campaign “Effective preparation – physical, emotional and intellectual – can have a huge impact on birth outcomes. It can significantly increase the likelihood of a normal birth and a healthy baby, and it can greatly enhance the satisfaction of the mother. Good preparation helps to prepare for the unexpected and can thus enable a woman to adjust herself and her expectations if circumstances change”.
So, learn about all your options, non-medical and medical (looks like you’ve already made a great start if you’re reading this). Ask questions. It really did help me avoid interventions and it helped me to prepare in case I did need any interventions, which I certainly would have if I hadn’t learnt about fetal positioning. Knowing fetal navigation techniques was like having a toolkit at my disposal which I could use to solve problems during my labours. It gave me a wonderful feeling of control and something to do and focus on during times of potential anxiety.

Yup that’s right, I did quite literally change the course of my two non-starter labours using the fetal navigation techniques I have included in Part 2 of this Guide – which to me was nothing short of miraculous – so I know firsthand that these tips are not a load of rubbish. This blog is not about bragging that I had good births. It’s about sharing so that other women can also have good births. It’s about sharing the fact that good births are very definitely possible. While I can’t even begin to understand the depth of feeling for those who have experienced traumatic birth – good births do happen and they can happen for you. Not only this but (without other complications), you can make them happen… if you know how.
My first baby wasn’t engaged even after several hours of early labour. The contractions were not increasing in length, strength or frequency. That can often be called ‘Failure to Progress’ and result in intervention such as induction/augmentation drugs and possibly csection. Not for me. I used a couple of the fetal navigation techniques in Part 2 of this Guide to Make Birth Easier and within minutes my labour switched into 6th gear – Strong, long contractions increasing in frequency – fantastic progress! Within a few short hours I gave birth to my baby in the birth centre pool without any intervention or drugs of any kind.
My second baby was back to back with stop/start and very irregular contractions for a week. Using one of the fetal navigation techniques in this Guide, I turned him around in an hour and regulated my own contractions, cancelling my induction appointment with half an hour to spare (there’s nothing like a deadline to spur me into action!). My second baby was also born calmly in the pool without any intervention or drugs, this time at home.
If only some of the secrets in this guide were not so secret, many other women could also increase their chance of a straightforward, intervention free labour and birth, if that’s what they would like. Most midwives don’t know about fetal navigation techniques – YET. This is why I founded #MakeBirthEasierCampaignUK the goal of which is, one day, to have all midwives trained in fetal navigation techniques as standard and be using them in routine maternity care, including antenatally. To achieve this we need clinical research to be done first (if any of you know researchers interested in doing a clinical trial please contact me!). Many midwives are already using the techniques unofficially with great results.
It’s never too early to start some of the techniques – even preconception. In general the physical preparation for birth should ideally be throughout pregnancy.
Why is Relaxation Important During Labour?
How on earth can you relax during labour? It hurts! Doesn’t it?
Annoying fact here (as mentioned above) – The more anxious or tense you are in labour, the more pain you’ll feel. Why? Fear in your body releases adrenaline which stops the release of oxytocin and therefore stops the release of painkilling endorphins into your body. There’s your smooth labour progress and natural painkillers cancelled right there. In addition to this, blood is directed away from your uterus, which is a muscle and needs blood and oxygen to function properly. The blood goes to your heart and legs instead because the human body is programmed to escape danger (fight or flight response).

© Warner Bros.
The organs needed for running away are prioritised by a brain experiencing fear. On top of all that, the tension you are holding in your body works against contractions. Tension in your uterus, cervix, and vagina literally holds on to your baby, just like squeezing your wee muscles works to stop your wee coming out. So let go. Take your body out of reverse gear and let your baby out.
Relaxing your mind and body literally reduces pain and allows labour to progress. It’s not hippy stuff – it’s biology.
I am well known by family and friends for being VERY easily stressed, so if I can RELAX, YOU CAN too.
Refer to Part 2 of this Guide to Make Birth Easier to find out HOW you can do this. I have listed lots of relaxation techniques there for you to choose from. I’ve also explained a little about Hypnobirthing below.
Basically find something that works for you in each stage of labour and use it, whatever it is. Everyone is different and has different preferences. You may have something else that you find helps you relax, so use that. Go with what works for you. Remember that labour is surprisingly intense and so whatever relaxation techniques you go for, have something fairly powerful up your sleeve for active labour and transition to keep you calm, focused and internalised.
Transition (where your cervix reaches its maximum dilation of 10cm and baby starts descending) is the time where many women have a bit of a panic and start saying things like “I can’t do it”. This is part of a hormonal switch happening and the panic feeling is normal if you are tense or in a lot of pain. The beauty of being calm is that you are much less likely to experience this panic, if at all, during the moments of transition. I was simply focusing on Hypnobirthing breathing techniques (described in Part 2 of this Guide) during my first labour, and at the moment of transition I felt the switch and calmly thought ‘wow that was it, I CAN do this’. That’s how powerful even just the breathing techniques are.
For my second labour we had got the hang of how to use the Hypnobirthing guided visualisation techniques we’d practiced. Using these, and light touch massage (a fab technique for reducing pain) I was so calm and internalised that when I felt the transition, I could sense exactly what my body was doing inside and I told my midwife matter of factly, “baby’s going to start coming down now”. Freaky but true. Her face was a picture – she was visibly startled! Even now I find it bizarre that I was like that. The usually easily stressed me – totally calm during the most intense moments of my life. Powerful stuff.

Hypnobirthing: It’s Not Hippy Stuff – It’s Biology
If you are reading this with a few weeks of pregnancy ahead of you I can really recommend Hypnobirthing (it’s basically relaxation techniques and birth education) as a fantastic way to help your mind and body relax during pregnancy and labour. It teaches you about the history and physiology of birth and reduces fear. It teaches breathing techniques and relaxation techniques so that your body can work the way it is designed to do. I used the Marie Mongan Method of Hypnobirthing for both of my labours with great effect. First labour I used only the breathing techniques and second labour I used the full range of Hypnobirthing techniques which I found incredibly powerful. There are a few different methods of hypnotherapy for birth out there to choose from including Hypnobabies, Natal Hypnotherapy and Wise Hippo, although I cannot make any comment about these others as I haven’t used them myself.
Check out this amazing youtube clip (Daisy’s Hypnobirth Homebirth Waterbirth) of a couple using Hypnobirthing. From about 12 minutes into the video there is a rare and wonderful example of one of the same Hypnobirthing visualisation/relaxation techniques we used for my labours. It is rare to see on video the couple counting out loud together to help mum relax. Many Hypnobirthing videos, although amazing to watch, don’t indicate what the mum is actually doing to maintain her calm, internalised state because she is so quiet. This video really shows how the visualisation technique they’ve practised together during pregnancy (which includes a whole relaxation script) instantly has an effect to help mum relax during labour. All he needs to do is count and, when she hears that counting, her body (having been programmed to relax during their practice sessions) automatically reverts to a relaxed state. Ridiculous as it sounds, and it does make me giggle every time I experience this – counting ’40, 39, 38…’ works to immediately relax me even now after more than four years – I feel all floppy!

If you don’t have time to fit in any Hypnobirthing sessions or other great birth education courses like Daisy Birthing (thedaisyfoundation.com), then breathing techniques are a serious winner in my book. Whenever I stopped working on my breathing I could feel the pain level rise. My husband cracked the whip reminding me when I lost focus, again and again, to work harder on my breathing and when I did work harder at the breathing, I felt the pain level go down again.
Combining focused breathing with counting while blowing my tummy up like a balloon was very effective and worked wonders for me. This was something I learnt through my Hypnobirthing course.
Part 2 of this Guide to Make Birth Easier explains the breathing techniques I used and when I used them.
No Purple Pushing Please
Tensing your whole body or holding your breath during contractions (‘waves’ or ‘surges’) does nothing to help you give birth. This is known as purple pushing and it will only make you very tired, very quickly. It is also more likely to cause distress to baby (from the temporary reduced oxygen), so if you are being monitored this can lead to a vicious cycle of attendees trying to make you push even harder to get baby out or even lead to interventions due to fetal distress and mum’s exhaustion. Purple pushing also increases the risk of trauma to your pelvic floor.
So how are you supposed to push? Part 2 of this Guide to Make Birth Easier explains what to do.
I pushed a lot harder than is indicated in the Hypnobirthing courses or videos (birth breathing/breathing your baby down), but I made sure my breaths were directed (by my own instincts) and any pushing was focused only in the right areas, not through my whole body. Do what you feel comfortable with.
If you feel the natural urge to push, go with it. I certainly couldn’t do anything about it when my body decided to go for it! Some women feel this urge before they are ‘fully dilated’ (although no one will know your dilation unless someone does a vaginal exam on you at that point which is entirely unnecessary if labour is progressing). Your body knows what it is doing. There is no evidence to show your own urge to push is a problem. Some women don’t feel the urge to push yet the contractions bring baby out. Follow your instincts.

Dilation
The cervix opens a little like a polo neck jumper does when a head is pushing through it. It softens, thins (effacement) and opens (dilation). It also moves to the front of the vagina.
Dilation is medically charted and used as a marker for how far along you are in labour. Dilation according to medical charts should progress by a particular measure per hour. If your cervical dilation isn’t increasing according to the graph it can be the reason for suggestions of hurrying things along using interventions.
In reality, human bodies and labours are all different and commonly do not do what charts say they ‘should’ do. A woman can be 3cm dilated for days and then zoom up to 10cm over a short period. A woman could also zoom up to 8cm dilation and then stay there for ages. Being in labour for a long time or being in painful labour and being told your dilation hasn’t budged or you’re only 3cm dilated can be disheartening and can slow down a labour even more.
There is no need to constantly check your dilation or fixate on it. Instead relax, move your body, and focus on your breaths and your baby coming. The length, strength and frequency of your contractions can give an indication of whether your labour is progressing well.
If baby’s head is pressing on the cervix at a favourable angle, descending and rotating as baby wants to, then dilation is likely to happen more easily. This is why fetal navigation techniques can help so much by aligning the head correctly through the pelvis.
Birth Plan for Vaginal AND Cesarean Birth
Write a birth plan (or birth preferences as I prefer to call it). Even if this is only so that you have researched and you and your partner understand the different options available, medical or otherwise, and what your preferences would be in different situations. This is called making fully informed choices. Weigh up all the options when deciding how and where you would like to birth.
I’m a realist. We don’t know how things will turn out (hence the term preferences rather than plan) so I prepared for all options just in case. If you do have a csection, it is possible depending on your situation, that you could make some requests so that things are a little more how you would like them. I wrote birth preferences, not only for a vaginal birth, but I also had one for a csection birth, just in case I needed one. This can make things more comfortable for you and can make birth easier for your baby even after the birth. There are some very simple things you can request that could make a great difference to your experience and to your baby’s health.
Part 2 makes a note on this and Part 3 of the Guide to Make Birth Easier is coming soon and explains how to write birth preferences for both vaginal and surgical births.
Use What You Learn
A gentle reminder here, that if you do decide you would like to try fetal navigation techniques, REMEMBER TO:
- practise them during pregnancy (even just once or twice will help),
- have the instructions with you to do them during labour,
- use them during early labour at home,
- ask your care providers if it is safe to wait while you try some fetal navigation techniques before resorting to intervention they may be suggesting.
If your labour does include intervention you didn’t plan on and you used the techniques and tips in this Guide, know that you gave it your best shot and you really did need intervention, instead of feeling like you were rushed into something early that maybe could have been avoided. Remember that if you or your baby are ever in danger, do what your care providers advise!
Out now:
Part 2 – Quick Guide to Make Birth Easier
Details of all my most useful hints and tips for easier labour – including those four key FETAL NAVIGATION TECHNIQUES that could prove so helpful.
Coming Soon:
Part 3 – Birth Preferences
- How to write your own birth preferences for vaginal birth, and
- How to write your own birth preferences for surgical birth for a more ‘gentle caesarean section’.
- What delayed or optimal cord clamping and skin to skin contact mean for you and your baby.
So watch this space.
Blog written by Alix Fernando
An extract of this Guide was published as a guest post on admissionsofaworkingmother.com April 2016 titled Make Birth Easier.
https://www.facebook.com/MakeBirthEasier
#MakeBirthEasierCampaignUK
The content of this blog is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.
Make Birth Easier Supports Optimal Cord Clamping

An excerpt of this article was published in
The National Childbirth Trust (NCT) magazine in December 2015.
‘Delayed Cord Clamping – The single most important gift you can give to your baby.’ Hannah Tizard #BloodtoBaby
Make Birth Easier
Blogging has been quiet for a few months since the launch of Make Birth Easier Campaign UK earlier this year, however, progress has not halted and with continuing support, the Campaign message – Fetal Navigation Techniques for easier birth, to be included in the standard training curriculum for all midwives – is reaching further and further around the world.
See below for links to previous Make Birth Easier posts including The Actually Useful, Very Sensible and Practical Guide to Make Birth Easier.
In this post, I focus on one of the greatest gifts you can give to your baby…
Optimal Cord Clamping – One of the Greatest Gifts to Your Baby
Pregnant for the first time and like many new mums, I had concerns about the health of my baby. Will she be born healthy? What can I do to give her the best chance of a healthy body and mind? Many mums find themselves dwelling on these and many other questions. Advice is plentiful and it can feel as if there are so many choices and considerations.
My Hypnobirthing teacher discussed several health topics with me including healthy eating, drinking plenty of water, appropriate exercise, and avoiding alcohol and caffeine. These are the basics of a healthy lifestyle of course and always advised during pregnancy. She also went through more specific options for our birth preferences including fetal positioning techniques to help labour progress more easily, different levels of monitoring available for baby during labour, limiting the number of vaginal examinations, and whether we would choose vitamin K by mouth or injection. I was very interested learning about these things and what they meant for me and my baby.
One particular thing she brought up which really caught my attention was Optimal Cord Clamping (OCC), also referred to as Delayed Cord Clamping (DCC). I had never heard of this before. I suppose it had never really occurred to me that anything different would or could be done with the umbilical cord other than the classic image I’d seen in movies and on TV. You will probably recognise the scene – where the cord has to be cut immediately as if it’s some kind of an emergency situation in itself.
So, doesn’t the cord have to be cut immediately after birth? Actually, in most cases, no it doesn’t.
Really?
This notion seemed very strange to me. If it’s not a necessity, then why on earth would it be done routinely for as long as many people can remember?
The procedure of cutting the cord immediately started in the 1960-70s with the introduction of drugs which reduce the incidence of post partum haemorrhage i.e. preventing the mum from bleeding significantly after birth. Great for mum – yes absolutely! Still, clamping and cutting the cord immediately was done with no consideration for the effect this would have on the baby and there is actually no evidence at all to support this practice today. It has become so normal that many presume it has to be done that way.
When I started asking questions, I realised that of course for the duration of its life inside mum, baby’s blood has been distributed between its body and the placenta. Research has shown that clamping and cutting the cord immediately means that one quarter to one third of the baby’s blood is left in the placenta and cord. WOW. That means that baby is missing up to 30% of its own blood and all the oxygen that goes with it. I was shocked!
I remembered donating a pint of blood and being told to rest for 15 minutes (or as long as I needed) with a drink and a snack before being allowed to get up and leave. That is just one pint of my blood. As a grown woman I usually have around 8-10 pints of blood inside me. I’m fairly tall so let’s say 10 pints. So I donated about 10% of my blood and looked rather grey and felt pretty wobbly. Imagine being born, at your most vulnerable moment in life, deprived of 30% of your intended blood volume… No wonder babies are often born in a weakened state!
My initial reaction was “I want my baby to be born with all its blood please!”
Then doubts came back to me…What if the cord is around the neck? Baby won’t be able to breathe! Then the realisation dawned on me during further discussion that baby doesn’t need to use its neck to breathe oxygen until the umbilical cord has been clamped. If the cord is pulsating, then the placenta is still attached and both the cord and placenta are still functioning; oxygenated blood is still being pumped around baby’s body.
The cord being around the neck once or even twice, it seems, is a fairly common occurrence, and while the cord is still functioning, this usually causes no problems. The message here is, if the cord is still pulsating, delay clamping and cutting while the cord is unwrapped from around the neck! Thankfully this is now taught in midwifery training, in some areas of the UK at least.
Of course there are cases where it might not be appropriate to delay clamping of the cord. These include; if the umbilical cord is compromised somehow, i.e. damaged or compressed, if the cord or the baby has a heartbeat below 60 beats/minute that is not getting faster, and also if mum is bleeding significantly (postpartum haemorrhage). These would be reasons to clamp and cut the cord early. In many other cases, if baby is struggling, it will benefit most from receiving more of its full intended blood volume.
If cord blood gases need to be taken, they can still be taken from a pulsating cord with a small needle. Levels of specific gases in cord blood can give an indication of the health of the baby and taking a sample from a clamped and cut cord is often standard procedure for high risk births. Doctors requiring a sample of blood gases is frequently stated as a reason for immediate cord clamping but gases can be taken from an unclamped cord. By using a small needle to take the sample (similar to when you have a blood sample taken from your arm), there is no need to clamp and cut.
A resuscitaire trolley called the ‘Bedside Assessment, Stabilisation & Initial Cardiorespiratory Support’ (BASICS) trolley was redesigned several years ago which now makes it possible not to have to choose between resuscitating a baby and delaying cord clamping. Resuscitation can be immediate and at mother’s side while the cord is intact which gives the baby potential for the greatest benefit. The team who redesigned the BASICS trolley received the Medical Futures Innovations Award in 2011 (Best Service Redesign in Cardiovascular Innovations) for their work on it. The BASICS trolley is called the Lifestart and has been produced by Inspiration. As more and more hospitals start to use the Lifestart trolley, many, many more babies will benefit.
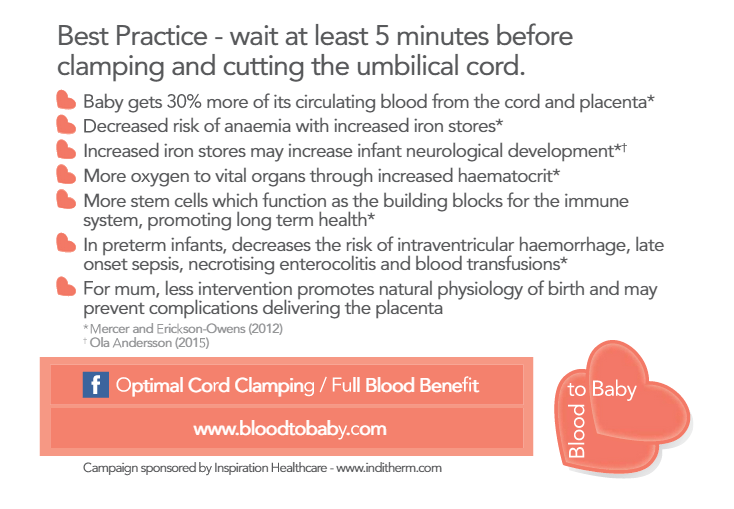
The benefits of Optimal Cord Clamping are many and include; improving the adjustment the baby’s heart and lungs make from being a fetus to being a breathing baby (because of the increased blood flow to baby’s vital organs in those first moments), improving iron stores up to 6 months, reduced instance of iron deficiency anaemia, higher red blood cell flow to vital organs, increased duration of early breastfeeding (I can only imagine this is due to baby being generally stronger from birth), increased white blood cells (leading to better infection prevention, including umbilical infections), less blood spatter (which in countries with high instance of blood borne disease such as HIV and malaria equates to prevention of disease transfer) .
 Research shows that babies can gain up to 214g in the first five minutes following birth if the cord is left unclamped. Cord blood has also been shown to contain a very high concentration of stem cells, important in development throughout the baby’s entire lifetime. There is a possible risk of jaundice which requires treatment by phototherapy and this must be weighed against the benefits of optimal clamping. Benefits for preterm and very preterm (premature) babies are huge. OCC leads to substantially lower rates of some life threatening issues.
Research shows that babies can gain up to 214g in the first five minutes following birth if the cord is left unclamped. Cord blood has also been shown to contain a very high concentration of stem cells, important in development throughout the baby’s entire lifetime. There is a possible risk of jaundice which requires treatment by phototherapy and this must be weighed against the benefits of optimal clamping. Benefits for preterm and very preterm (premature) babies are huge. OCC leads to substantially lower rates of some life threatening issues.
For the mother, optimal clamping does not increase the risk of postpartum haemorrhage. Allowing the umbilical cord to stop pulsating also contributes to the placenta being able to detach from the uterus more safely and efficiently, so this in itself reduces the chance of significant maternal bleeding. Interestingly, early breastfeeding is also known to help the placenta to detach properly and to reduce the occurrence of bleeding from mum. Many midwives are waiting until after the cord has stopped pulsating to administer the hormonal injection (usually syntocinon these days) which helps the placenta be born more quickly as part of an actively managed third stage of labour.
There is no reason why, in most cases, OCC cannot occur also as part of a caesarean section too. Baby can be placed between mums legs for vital skin to skin while the umbilical cord is allowed to complete its job. This also helps baby be exposed immediately to mums good bacteria, so important to help baby build a strong immune system (‘Seeding the Microbiome’, which uses mother’s natural healthy bacteria -from vagina, skin to skin and breastmilk – to colonise the baby’s gut, as would be the case for a vaginal birth, is a subject worthy of a whole article all of its own so watch this space!).
So why in many hospitals is the umbilical cord still being cut immediately as a matter of routine? The truth is, it has been a very long battle to gain recognition of the benefits of delaying clamping of the cord to allow placental transfusion. Due to much campaigning by some amazing midwives and doctors from the UK and around the world, thankfully there is now extensive evidence available for both term and preterm babies, and recognised international and British bodies such as the World Health Organisation (WHO), the International Liaison Committee on Resuscitation (ILCOR), the Royal College of Midwives (RCM), and the Royal College of Obstetrics and Gynaecologists (RCOG), in addition to the National Institute for Health and Care Excellence (NICE) Guidelines now include for Optimal Cord Clamping.
British and international guidance now recommends that the umbilical cord should be left intact for at least a minute based on a clinical assessment of the situation. Since 2014 the NICE Guidelines make this recommendation unless there is a concern about the integrity of the cord or the baby has a heartbeat below 60 beats/minute that is not getting faster, which is very rare.
Many hospitals are changing their procedures to include at least some delay in clamping the umbilical cord, although it is still taking time to filter through. There are not yet that many hospitals with specific OCC guidelines in place and there is still a lack of evidence based recommendations for the timing of umbilical cord clamping. Hospital guidelines range from 1, 2, or 3 minutes and some allow the cord to stop pulsating. In other hospitals OCC is something you, as mother, need to state as part of your birth preferences.
As an example, my own birth preferences (otherwise known as a birth plan) stated the following: ‘DELAY CORD CLAMPING and cutting for minimum 3 minutes or UNTIL AFTER PULSATION HAS CEASED (unless baby’s heartbeat <60bpm without increasing, or, there is significant maternal haemorrhage). If cord gases need to be taken, please do so with a small needle so delay in clamping can occur. In event baby is compromised she will benefit most from receiving placental blood transfusion. If the cord is pulsating, the placenta is still attached and both are still functioning’.
One of the barriers to Optimal Cord Clamping not yet being routine in hospitals is that some hospitals have interpreted that OCC is only suitable for healthy women and not suitable for any women categorised as ‘high risk’. This is due to the NICE guideline on OCC being included in the section for healthy women and babies. Hospitals can have rigid policies for categorising women and consequently may practice Immediate Cord Clamping (ICC) on healthy women and babies who have been given a ‘high risk’ label (induction, Vaginal Birth After Caesarean, continuous monitoring…). Research shows OCC presents no risks to women, whether high risk or low risk, and it actually benefits compromised babies. It is precisely these babies who are struggling that frequently need Optimal Cord Clamping even more in order to give them the strength to recover or even survive. Immediate Cord Clamping is not evidence based. Whatever category women fall under it is important for women to tell their birth attendants that they want their baby to have Optimal Cord Clamping.
One British Consultant-led Midwife Unit introduced Optimal Cord Clamping guidelines for ALL babies, regardless of delivery and included for a team of Advanced Neonatal Nurse Practitioners (ANNP) to work with the midwifery/obstetric teams to ensure benefits from OCC. The Unit conducted a review to see if these guidelines were being put into practice. The findings were startling. The introduction of OCC resulted in a significant reduction in the number of babies born there receiving resuscitative measures at birth. The Unit very much supports the practice of ‘assisted transition’ from placental to pulmonary respiration (transition from oxygen via the umbilical cord to breathing with the lungs). In short – delaying the clamping and cutting of the cord means that fewer babies need help to breathe.
The miracle moments of birthing my daughter, and then my son, into water, brought home to me the still ingrained fear I had of the baby needing to breathe immediately. Both were under water for what seemed like an eternity. First the head was born, then each baby took a minute or so to turn to allow the body to be born. During these few minutes under water the previously held anxiety in me reared its head for a moment that baby needed to breathe, but of course, in reality the baby is absolutely fine underwater (as I was reassured by my lovely midwife). It has spent the whole of its life inside mummy in fluid and never yet used its lungs. For both my children I chose to delay cord clamping until the umbilical cord had stopped pulsating and was empty and white #Wait4White.
It is now recognised that best for baby is to give it time to start using its lungs properly before the cord is clamped (assisted transition). Give it time to receive its full quota of oxygenated blood. Baby will be much stronger for it in those first few vulnerable moments of life after birth. Incredibly, this fact has been written about by scholars for thousands of years. Aristotle 300BC “Frequently the child appears to be born dead or it is feeble but before the tying of the cord, a flux of blood occurs into the cord and adjacent parts…and at once the baby, who had previously been as if drained of blood, comes to life again.
Optimal Cord Clamping saves lives. Share this message.
Blog written by Alix Fernando – founder of Make Birth Easier Campaign UK. https://makebirtheasier.wordpress.com/ https://www.facebook.com/makebirtheasier/
#MakeBirthEasierCampaignUK #SpinningBabies
With very special thanks for the assistance of Amanda Burleigh – Optimal Cord Clamping campaigner, SHCR Change Agent, OCC/Full Blood Benefit Facebook page founder and Midwife of the Year for several years running with various bodies including the British Journal of Midwifery. Medical Futures Innovations Award in 2011 for BASICS trolley with the basics team. See also #Wait4White.
For further information please see Optimal Cord Clamping campaign #BloodtoBaby by Hannah Tizard, RCM shortlisted Evidence into Practice Award 2016, UCLan student midwife, National OCC Working Group member. Order free educational resources for midwives, childbirth practitioners, women and families from www.bloodtobaby.com
Make Birth Easier Blogs
1. Click here for the story behind the Make Birth Easier Campaign and find out about how I used fetal navigation techniques to have two straightforward, intervention-free labours against the odds.
2. Click here to learn more about the research we so need into fetal navigation techniques to prove they are safe and effective.
3. Click here to learn about how moving mummy helps baby to move into a better position for easier birth and how the medicalisation of birthing over the years has ignored gravity and movement.
4. Click here to read about the dramatic difference that using fetal navigation techniques for easier birth can make to thousands of women by reducing the need for aftercare, both in terms of post operative care, and also mental health issues such as Post Natal Depression (PND) and Post Traumatic Stress Disorder (PTSD).
Make Birth Easier blog written by Alix Fernando – founder of Make Birth Easier Campaign UK.
https://makebirtheasier.com/ https://www.facebook.com/makebirtheasier/ @MakeBirthEasier #MakeBirthEasierCampaignUK #SpinningBabies
The contents of this blog are not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or your recommended routine.
Make Birth Easier Campaign – After Care (Featuring A Personal Story)

‘Fetal navigation techniques can facilitate easier, faster and safer birthing thus reducing the ever increasing number of caesarean sections performed and the amount of drugs administered. A reduction in medical intervention, and particularly caesarean sections, would reduce the necessity for aftercare; helping to cut down on post operative infections, post operative complications, and even helping to reduce the occurrence of post natal depression and post traumatic stress disorder.’
The Story So Far
1. Click here for the story behind the Campaign and find out about how I used fetal positioning techniques to have two straighforward, intervention-free labours against the odds.
2. Click here to learn more about the research we so need into fetal positioning techniques to prove they are safe and effective.
3. Click here to learn about how moving mummy helps baby to move into a better position for easier birth and how the medicalisation of birthing over the years has ignored gravity and movement.
It has now been three weeks since the launch of the MakeBirthEasierCampaignUK and with continuing support, the Campaign message – fetal positioning techniques, such as those on SpinningBabies.com, to be included in the standard training curriculum for all midwives – is reaching far and wide.
A Personal Story Shared
Laura attended a Positive Birth Movement meeting in the hopes of building her confidence for her second labour which was fast approaching. This is where I met her. I was attending the group as a speaker for fetal positioning techniques I had learnt on SpinningBabies.com. She had already taken affirmative action by joining the Daisy Foundation (empowering education and support from pregnancy to parenthood) for a course, and this meeting was her next step on the road to recovering from her first labour experience.
As Laura started telling her story, I could immediately feel her anguish as she welled up and had to pause for a second to compose herself.
Laura had had a back-to-back baby and also been very poorly at the time of going into labour. She’d not had the chance to labour fully as she’d been told she would be prepared for a caesarean section to deliver her baby.
The anaesthetist doing the epidural, for some reason vocalised what he was thinking and stated more than once that it was difficult to find a suitable injection site, and that he couldn’t get the needle in the right place.
Laura was terrified that she would be left paralysed by this procedure going wrong and felt utterly helpless to do anything about it.
Following the delivery of her baby girl by csection she found it very difficult to bond with her baby due to the traumatic circumstances she’d experienced at the birth. She was overwhelmed with negative emotions and guilt, and this only amplified her trauma.
Here she sat in front of me, three years after the experience, crying her heart out, because the birth of her first child had been taken from her. She had not been allowed to give birth vaginally. Not only that, but she had been terribly traumatised by the experience which had filled her with fear.
My Reaction
I’d also had a back-to-back baby, yet I’d managed to turn him around and regulate my own contractions to enable me to have a smooth, intervention and drug free birth. Why, I wondered, are women and midwives not aware of the techniques I used? Laura could have had a much more positive birth experience had she known about fetal positioning techniques. It absolutely breaks my heart to see women go through such negative birth experiences, especially when, in most cases, there are alternatives. Malposition or malpresentation do not have to automatically mean a medicalised birth.
I told the group the stories of my two very straightforward labours which, without fetal positioning techniques could have easily involved induction, augmentation, assisted delivery and/or csection. I share my stories to help people understand the possibilities available to them. They have options. If I can do this, maybe you can benefit too. You at least have a much better chance of the birth you hope for.
We talked about several different fetal positioning techniques and what they’re used for. We talked about the feelings of empowerment created by having options to choose from. Many times I’ve described it as having a toolkit from which to draw whatever tools are required for the job at hand. This to me was both empowering and calming. It seems I’m not the only one.
I Had My Little Boy
Here is the story of Laura’s second labour, in her own words…
“I had a fantastic birth experience.
I had a long early stage at home and then had my 41 week antenatal check at the hospital. I described my contractions and we agreed I would be admitted as I was 1cm and feeling like I wanted some support: I felt a little like history was repeating itself. I’d had a little wobble as it had been stop start for quite a while by then despite me being active, changing position and using all my new-found knowledge.
I pulled myself back whilst we waited for a bed on the ward. Once I’d vomited a bit, replaced some fluids and found my calm, things quickly heated up. Contractions got going and I was transferred to the labour ward. Initially the midwife was not my cup of tea and despite me telling her repeatedly that the CTG wasn’t working, she just kept saying my contractions were too weak and may as well have patted me on the head when I said they weren’t and were very strong. I checked the clock and knew it would soon be handover and ignored the silly woman when she told me off for hyperventilating. She actually made an audible snort when my partner explained the escalator breath to her.
Handover 30 mins later… In walked a fantastic midwife and student midwife and things quickly changed. She changed the lead on the CTG and my contractions suddenly warranted a big gold star for mummy’s coping! Got all the lights dimmed, LED candles out, essential oils and Daisy music on.
Over the next 5 hours I progressed fantastically. Changing position: in the zone; calmly labouring. The midwives were so supportive and held the CTG in place if I wanted a position that wasn’t lending itself to the monitoring.
My waters went and things stepped up a gear further. Vaginal exam at midnight, I think, and 6cm! I was so happy and quite high on gas and air. At about 02:15 things suddenly changed and the contractions were instantly unbearable. We moved positions a couple of times. Tried a few things but with every contraction came this awful pressure and then baby’s heart rate started diving very low. We quickly got a clip on his head and had a look at what was happening. He was somehow stuck and I can’t remember much of what was said from this point, but from then on his heart was nearly stopping with each contraction. Everything slowed down and I just became very calm. I knew we were off to theatre. I smiled happily as they put the spinal in and had the most serene Cat 1 csection anyone has ever had!
His head was a very peculiar shape where he’d been squished!
I feel like I’ve had a triple victory somehow with this birth.
Firstly, my body was doing it! Gas and air, tens and breathing.
Secondly, I’ve truly healed from my daughter’s birth emotionally, and thirdly I had a spinal and a csection – two things that have brought me out in cold sweats and nausea for the past 3 years – without even a second of panic or fear. I knew it was all going to be ok.
The icing on the cake was overhearing my midwife telling another midwife about how fantastic I was and how much she enjoyed my labour!
So as I sit here feeding my handsome baby boy, I’ve come to reflect on my journey. I never knew I was so strong, I never knew I could heal my own wounds and I never knew how wonderfully positive any experience can be.
Thank you to everyone who has helped me on my journey. I am very grateful for all of the support I’ve been given and hope to give back to others in the future.
Love, a very euphoric (if a little sore) Laura xx”
Achieving a Transformative Experience
Before her second labour, I‘d sent Laura a copy of the csection birth plan I’d prepared for myself in case things didn’t go as I hoped. I asked Laura, if this birth plan had proved useful and how she’d tackled the csection. The following is her response:
“I actually went for a pretty medical csection and unusually requested that I didn’t hold my baby immediately. The reason for this was that in the lead up to birth I went through all the individual things that heightened my anxiety last time, so that I could stay as calm as possible. One of the things that terrified me with my daughter’s birth was when she was placed on my chest, I felt like I was going to drop her as the spinal block made me physically shake. I knew worrying about this could be a trigger for a panic attack so I asked that I wasn’t given her to hold until I asked, and that she went straight to my partner. This was followed to the letter. He held our little boy and bonded with him until I felt stable enough to do it.
I had a strong fear of epidural so the hospital had arranged in advance for me to have an appointment with the head anaesthetist and talk over my fears. When I had an epidural with my daughter, the man that did it mentioned a couple of times that it was going to be difficult and may take more than one attempt – I had a panic attack over this and high anxiety whenever I thought about it for the 3 years until I dealt with it.
The lady I met with was fantastic, examined me and felt my spine, as I was scared it was abnormal and therefore I would be paralysed if I had an epidural. My back is normal, and she suggested as I was so tense I may not have lengthened my spine enough and he was just speaking aloud his internal monologue rather than suggesting I could help in some way by loosening up.
The anaesthetist went through my fears one by one, and addressed all of them. She then wrote a letter for my notes telling them not to offer me an epidural (I also wrote this in my birth plan) and that in the event of an EMCS (emergency csection) I could have a spinal. This was definitely read by all concerned at the time and they were incredibly sensitive. I used my Daisy Birthing breath (in for four, out for eight) to remain calm and it all went fine.
Also, I didn’t want the screen lowered as I was scared of that.
Basically I went through everything I knew I could have and weighed up what scared me first time and how I could keep calm this time – even if that meant going against the more natural section most VBAC (vaginal birth after csection) women want. This was a time for learning from things. I tried so hard to do things “properly” last time and put too much pressure on myself. This time I listened to myself. I’d learnt so much about me, and only did what I knew I could cope with.
Other things I put in my birth plan were also respected, such as lowering of the lights, listening to my Daisy music, using lavender and clary sage spray in the room near me and -most importantly for me – not to be offered pain relief or for the word pain to be used. My midwife was fantastic!
I didn’t use Spinning Babies in the end but used the “rotate to dilate” movements I’d learnt with Lorna Brown at Daisy. I used pelvic tilts and the “camel walk” to engage him.
I spent a lot of my labour on all fours, gently circling my hips clockwise with each contraction and breathing. I later heard my midwife telling a colleague (when she didn’t know I was in earshot) how incredible I was and how peaceful and calm it was.
Another fab thing that happened was that I later saw the anaesthetist on her rounds (who’d given me the talk) and she recognised me. She was over the moon to hear that she really had helped and was noticeably touched that she’d made such a difference.
Near enough every health professional I came into contact with listened to and respected my views and I believe largely because I was so informed but also as I am naturally a gentle negotiator, and tend to get my own way with knowing how to strike the right balance between being firm and being gentle. It seems to work for me!
My enthusiasm seemed to rub off on people. I know I was lucky though, as I do hear a lot of consultants can push their own agenda onto mothers.
I cannot praise the hospital enough for the support they gave me.”
The positive experience Laura had with her son’s birth was helped a huge amount by the kind and thoughtful treatment she received from the medical staff involved in her labour and the way they responded to her birth plans. Communication and kindness go a very, very long way towards a positive maternal experience!
Empower Yourself with Knowledge and Preparation
I wanted to include Laura’s story in my blog for several reasons.
It has been an incredible journey for her from the way she felt about her first birth, to her second which was a hugely transformative experience. From negative to positive because she took control the second time. She empowered herself with knowledge, preparing herself for different eventualities. She worked at making it her own birth and finally, with a csection she was at peace because she knew she’d put in her best effort and the section was a medical necessity for the health of her baby boy. Her birth was not taken away from her this time. It was hers and powerful and positive. This changed her emotional response dramatically and she bonded well immediately.
**Inherent in my campaign is the concept of helping to empower women in their births so that, regardless of how their baby is eventually delivered, they know they were informed. They were aware of the array of options available and made use of them – this can make a huge difference to the birth experience postnatally.**
The positivity in Laura’s story I hope will speak volumes and it’s a wonderful and amazing example of what this campaign is trying to achieve. Her journey has really touched me.
Saving Pain and Money
In this blog I wanted to highlight ways of helping to reduce the number of women going through negative birth experiences and thereby reducing aftercare required, both psychologically and physically.
So many women are affected by post natal depression (PND) and post traumatic stress disorder (PTSD) due to their negative birth experience and the physical recovery they endure postnatally. Time and time again I hear stories similar to that of Laura’s first birth: stories of fear, pain, loss of control to a medicalised system and emergency csection. Women wondering if they could have birthed their baby differently if they’d known x, y, z , or been ‘allowed’ more time (a woman’s informed choice in all this is a subject which I think needs discssing in its own right, so I won’t go into it here).
If midwives are trained to recognise signs of fetal malposition and can support a labouring woman by applying specific fetal positioning techniques to resolve these malpositions, the 25% csection rate in the UK (yes that’s 1 in 4 women) could be reduced to a more acceptable 10-15%, as recommended by the World Health Organisation back in 1985 and again in 2015. This lower more acceptable will remain because – regardless of balance, movement and specific positioning techniques – sometimes, csection is the safest and sometimes the only option for the health of mother and baby. Fetal positioning techniques are not a guarantee in any labour, but they do give a much better chance of minimising interventions.
Csections increase the length of time spent in hospital in general and increase the risk of admission to the Intensive Care Unit for baby and also for mum.
Caesarean section is not an easy option. It is major abdominal surgery with its own inherent risks and associated fears. It is higher risk than a vaginal birth, with complications including post operative infections, blood clots and postpartum haemorrhage amongst others, and a range of side effects from the epidural or general anaesthetic such as nausea (for which anti-sickness drugs can be administered), low blood pressure (for which blood pressure medication can be provided), allergic reactions, chest infections, and in rarer and more serious cases, damage to nerves or the surrounding tissues at the epidural site.
Add the above complications, all requiring medical treatment, to the many occurrences of PND and PTSD requiring psychological evaluation and treatment such as Cognitive Behavioural Therapy, and there is already quite a list.
Research now shows that babies born via csection may miss out on an immensely important part of vaginal birth – seeding the baby’s microbiome. This is where the baby is exposed to the mother’s own bacteria within the birth canal, during immediate skin to skin contact with the mother and breastfeeding, helping the baby’s immune system to develop to its full potential, and providing the infant with a reduced risk of developing one or more serious diseases later in life.
There has also been a stark warning recently by Dr Michel Odent that increased induction/ augmentation (use of synthetic hormones to start or increase strength/frequency of contractions) rates are suppressing the naturally occurring hormone oxytocin, which could affect the natural release in the body and have adverse effects on birth and breastfeeding.
Speaking from a business perspective, collectively reducing the occurrence of the above complications by eliminating a significant percentage of augmentation, csections and negative birth experiences, this could save a huge amount of money for the NHS and help ease pressure on midwives in so many ways. The range of aftercare for birth, particularly births that end in csection, is huge and is very costly to the already overstretched NHS. More importantly, reducing these would save a lot of pain for women!
I’m sure the NHS would like to see a positive difference in the number of women leaving the labour ward with a happier, easier outcome.
The Next Step
Step 1: Generate interest and support from mums and the midwife community. This bit is continuing well and the campaign is being followed by more people each day.
Step 2: Generate interest and support from the research community. The interest we received into doing research into fetal positioning is still keen and the facility is open to doing a study…with, as I suspected, a couple of hurdles standing in the way – hurdles which I have already covered in previous blogs. This facility needs an evidence base with actual data behind it first to show that it’s safe and it actually works before doing a larger trial: fair enough really. So we’re back to the following (click to refer to my second and third blog posts which cover these in more detail):
• Case reports – observational data on volunteering patients – tracking labour and delivery outcomes, safety, any adverse effects and compare with a control group.
• Cohort/small pilot study into safety/efficacy, again with consenting individuals.
• Pending results from the first two studies, a randomised trial could be done.
It may be unrealistic to expect to generate direct evidence of the impact of fetal positioning techniques on labour outcomes, due to the number of compounding factors. However we would hope such studies could support a trend towards improved outcomes.
I imagine there would need to be an obstetrician involved at some point?
Finding a willing researcher is a great step for the #MakeBirthEasierCampaignUK in such a short time – there’s still a very long way to go. With continued support to raise awareness about fetal positioning by sharing the campaign message, we hope this first step becomes one of many.
Step 3: Generate interest and support from the obstetric community. I have received some support here which I believe to be crucial to these techniques being accepted into mainstream care.
Step 4: Generate interest and support from the medical press. I’ve begun tweeting the medical press and can tentatively say I’ve had a couple of journalists and editors follow @MakeBirthEasier.
This is such a complex and dynamic subject. Any advice or guidance you clued up people out there (researchers, midwives, obstetricians, gynaecologists, scientists, anyone in the know!) can offer on any of these questions would be very welcome. All comments which have come my way so far have been valuable and I would like to thank all of you who’ve been in touch!
If I can use fetal positioning techniques myself for both my births with such impressive results (see my first blog post MakeBirthEasierCampaignUK dated 11 May 2015), imagine what trained midwives could achieve using them every day. Women in this country would have a better chance of an easier, uncomplicated, intervention free birth if midwives and other health care providers had training in fetal positioning techniques. To reach that goal, we need evidence and support.
This is a huge opportunity to invest in a more positive future for maternal care in the UK. I am hopeful that I have your support.
For health professionals and others interested in being part of this opportunity, please leave comments / advice / guidance / offers of funding / offers of research team & research facility (!!) on this blog page.
You can also contact me via my page at https://www.facebook.com/MakeBirthEasier (particularly if you would like to message me privately)
The Campaign is also on Twitter @MakeBirthEasier, #MakeBirthEasierCampaignUK
Blog written by Alix Fernando
The content of this blog is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.
Make Birth Easier Campaign UK – Move Mummy to Help Baby

‘Please don’t forget maternal position, the obstetric bed was probably the worst invention in the history of childbirth, turning women into passive patients who expected that there was nothing they could do to reduce their pain. MJ’
Campaign Update
If you haven’t read my first blog post yet – the story behind the Campaign – click here. The second blog post focused on the research we so need into fetal positioning techniques to prove they are safe and effective. Believing in them because so many people have used them to great effect does not clinical evidence make… Click here to read about research ideas.
It has now been two weeks since the launch of the MakeBirthEasierCampaignUK and support has continued to grow. After I published my second blog post, it had 400 views in one day. I don’t know if that is good in the world of blogging for a second post but I thought it was pretty fantastic! The Campaign message – fetal positioning techniques, such as those on SpinningBabies.com, to be included in the standard training curriculum for all midwives for use as part of routine care – seems to be making its way around the world at a steady pace, reaching many countries including the UK, USA, Australia and as far afield as Bermuda and the Philippines!
I have had many supportive comments, “I love what you are wanting to achieve and yesterday I shared on both my FB page and website. It is a massive project and you will face many many challenges…” and some very constructive advice and suggestions which I will be covering below.
Move Mummy to Help Baby
Thank you to Margaret Jowitt for your comment ‘Please don’t forget maternal position, the obstetric bed was probably the worst invention in the history of childbirth, turning women into passive patients who expected that there was nothing they could do to reduce their pain.’
You have inspired the blog this week!
Firstly, I may not have been clear in one vital part of my explanations of fetal positioning techniques. Fetal positioning can be improved by ‘maternal positioning’ and posture. The techniques on SpinningBabies.com use ‘maternal positioning’ in order to achieve optimal ‘fetal position’. Move mummy and this can help baby to move.
Secondly, to the obstetric bed. The obstetric bed is great for the care provider who has a better view of, and access to, ‘proceedings’. ‘Proceedings’ for the labouring mum in this position however are far from ‘better’. Lying on ones back, particularly with legs up in stirrups, is the worst position! The medical term for this is the lithotomy position and it is a common position used for medical examinations and surgeries involving the lower abdomen and pelvic area. References to the position have been found in some of the oldest known medical documents including versions of the Hippocratic Oath!
However popular it has been with obstetricians, the position is not conducive to a smooth labour as it constricts the birth canal, puts pressure on the coccyx, and does not allow the mother to move during the process, therefore increasing pain in labour. During labour, the position appears to cause compression of the main maternal blood vessels including the vena cava, thereby reducing the flow of blood to the infant which can cause severe problems for mum and baby.
The baby is pulled by gravity into the mum’s back rather than out and the birthing process is much less active. It becomes, as Margaret quite rightly put it – ‘passive’ birthing. This makes for much more effort on the mum’s part and, I’m to understand, considerably more discomfort. Passive birthing also often requires more invasive medical interventions, and is associated with increased trauma to both mum and baby.
Even the World Health Organization does not recommend the use of the lithotomy position for child birth, and states that ‘Giving birth in an upright position appears to be associated with several benefits, including reduction in the duration of the second stage of labour. Pending further confirmation of these benefits women should be allowed to choose their birthing position.’
My mum gave birth to three of us in the lithotomy position and has stated categorically that if she knew then the things that I have taught her about birthing and the role of movement and gravity in labour – she would never, ever, have given birth the way she did!
Misdirection
The strange thing is these days, that even though movement and remaining active is readily promoted by midwives antenatally, it is all too easy for a woman in labour to walk into the labour room and be guided directly to lying down on the bed. Why does this still happen? It is ingrained in us, by media and society in general, that a labouring woman is supposed to lie down on her back. ARGH!
Luckily I know a few midwives making efforts to turn this initial error on its head (pardon the pun). Some midwives are leading the labouring mum into the labour room but sitting on the bed themselves so the woman in labour could only sit on it and cannot lie down on it. They may even move the bed to one side of the room rather than it being a centre piece, so that space is made available for the mother to move around, maybe sit on a birthing ball, or put pillows on the floor for her knees so she can lean over the birth ball or against the side of the bed…
Hang on, did I say bed? Yes, okay, if we are a bit more inventive, there are some pretty good ways we can make use of the obstetric bed, it has to be said. The hospital bed has a back that raises up at an angle so mum can lean forwards over it while on her knees. Another rather smart use of the modern obstetric bed is that the lower section can be lowered in a kind of step fashion which is a fabulous shape for doing the classic Spinning Babies ‘Forward-Leaning-Inversion’!
Is All this Extra Training Really Going to be Used?
The other night I had a chat with an ex-midwife in her 70s who is very close to me. She is very supportive of this Campaign, yet still has her doubts about the practicalities of its use in certain settings and she played devil’s advocate with me to press home some points.
In the home birth setting or a small Birth Centre with enough midwives to go around, yes there may be plenty of time to spend with the labouring mum, one to one. In these situations a midwife can invest the time required to do fetal positioning techniques. Some take a few minutes and some, for example the ‘Abdominal Lift and Tuck’, need to be done through 10 contractions. Hmmm…alarm bells…10 erratic contractions for me with my back to back baby No2 took well over an hour – maybe even an hour and a half. Am I saying that a midwife needs to spend an hour and a half with a mum to do just one exercise?
Midwives Stretched to Limits
Now let’s look at a busy labour ward in September or October – notoriously the busiest months for number of births. This is the time when a midwife is popping in and out of the room and may be gone for what feels, to the labouring mum, like a million years. Where does she keep going? Why does she keep leaving the room?! Well, she has several other ladies at various stages of labour, with varying degrees of urgency to attend to. This is the reality. One to one care at this point is not what it feels like to the patient left with her hubby or relative or at times – alone. The midwife cannot leave a woman who is in the midst of actually delivering a baby or placenta to spend time with the lady who is experiencing a long labour with contractions which for one of several possible reasons, are not increasing in strength. Maybe this is due to stress of being without a midwife!
Whose fault is this? Let’s not go into that here but it is not usually the fault of the midwife, we can safely say that! She (or he), is stretched beyond sensible limits probably far too often and is trying her level best to get through the shift doing a great job of bringing babies safely into the world.
Maybe this failure to progress is due to a malpositioned baby. So let’s say the #MakeBirthEasierCampaignUK is entirely successful and midwives are now all being trained in fetal positioning techniques – where then is this trained up midwife? Why is she not on hand to come and spend that hour and a half with this lady to do an ‘Abdominal Lift and Tuck’? Because it takes too long and she is away tending to a more urgent labour! This was devil’s advocate talking.
My answer to this quandary is that actually, and I must make it abundantly clear here, it would NOT necessarily need to take an hour and a half of the midwife’s time to do the ‘Abdominal Lift and Tuck’. It could take a couple of minutes to explain how to do it to the mum, and guide her into the correct position for contraction number 1. Then the midwife could go and see her other patient/s leaving mum coping quite well with the other 9 contractions needed for the ‘Abdominal Lift and Tuck’. I did this exercise on my own without anyone to help me. I left my husband sleeping soundly in bed while I carried it out according to the instructions on the website.
May I add here that taking some form of action to actively improve the labour, immediately gives a feeling of empowerment, which is incredibly good for a birthing mum psychologically, and subsequently physically.
Again, another staple of Spinning Babies like the ‘Side-Lying Release’ – which in labour is held through 3 contractions – could take just a few minutes of the busy midwife’s time while she helps to position the mum on her side in the correct manner, gives instructions to the mum and birth partner (husband, relative, doula) and leaves them to continue after the first contraction.
These are possibilities. Depending upon the technique in question it could be fine to leave a lady doing an exercise without the midwife present throughout. After all, a birthing ball is readily accepted as something a mum can use without the attention of a midwife. Or should the mum go back to lying on her back on the bed…
Taking More Time to Create Time
The point I am trying to make (hopefully this is making some sense!) is that investing a few minutes, even on a busy labour ward, to use these fetal positioning techniques where appropriate (where a midwife assesses that it would be beneficial), can shorten and ease labours, and reduce the number of interventions, augmentations, assisted deliveries and csections. Mums (even very tired ones) could be motivated to do them to avoid these interventions and eventually, when the techniques become a routine, standard part of everyday midwifery, time will have been created – created by a reduction in the number of interventions – created by a reduction in the number of emergency csections – created by a reduction in the time each woman is in labour in the first place – a less busy labour ward. Even if it is just a bit less busy, and there are just a few less interventions, won’t this make a big difference in the number of women leaving the labour ward happier, having had an easier time and better outcome?
In fact, I wrote the above text last night, and tonight during my review, I have found information via the World Health Organisation as follows – ‘the potential to improve delivery outcomes; reduction in the duration of second stage of labour may help reduce overcrowding in labour wards and reduce the time health-care providers spend with each woman.’
It appears I may not be as daft as I look…I should run this by my friend the ex-midwife! The text is in particular regard to allowing women to deliver in an upright position, however, it refers directly to reduction in the duration of second stage of labour, which fetal positioning techniques help to achieve. This is what I am hoping will happen by implementing fetal positioning techniques across the UK. Fingers crossed midwives!
Antenatal Preparation
Something that would add a lot to the use of fetal positioning in labour, is the use of fetal positioning in pregnancy. If women are using these techniques to balance their uterus, ligaments and muscles before labour even starts, many malpositions and malpresentations could be prevented in the first place. Plus if fetal positioning techniques are then required during labour, women would already be familiar with the techniques and the time midwives need to spend guiding them during labour could be shortened even further. After all, midwives are not integral to the hypnobirthing process and are not required to be present to monitor that are they. If women are adequately and routinely prepared with fetal positioning knowledge and practice, they could possibly go ahead and do these exercises themselves with just reminders or pointers as to which exercise would be beneficial for whatever situation arises.
The Next Step
So two weeks in, what is the next step? My plan is progressing rather better than I anticipated…
Step 1: Generate interest and support from mums and the midwife community. This bit is continuing well and on Facebook and Twitter there are more and more liking and following each day. Today @MakeBirthEasier topped 100 followers on Twitter!
Step 2: Generate interest and support from the research community. Can I just put a BIG FAT TICK by this one as the Campaign has received keen interest to do some research!! Although it is not yet known if we can pursue this avenue, it is incredibly heartening to know that there are researchers out there who may have the means, and are eager to study the effect of maternal / fetal positioning techniques on birth outcomes. This is already a huge step for the #MakeBirthEasierCampaignUK in such a short time – there is still a very long way to go. With continued support to raise awareness about fetal positioning by sharing the campaign message we hope this first step becomes one of many. Totally buzzing with excitement at the possibilities!!
Step 3: Generate interest and support from the obstetric community. I have started to receive some support here which I believe to be crucial to these techniques being accepted into mainstream care.
Step 4: Generate interest and support from the medical press. I have begun tweeting the medical press and can tentatively say I have had a couple of journalists and editors follow @MakeBirthEasier.
Further Thoughts on Research
My last post set out some thoughts and ideas on research methodologies. I’m over the moon about the possibility that there is a researcher who may be able to set up a study at their facility. It is immense news! We can only keep our fingers crossed that there is a viable study to be pursued. We will have to wait and see if we can get approval!
This however is certainly not where we put our feet up – we cannot rest until our goal is achieved! There are many avenues to look down, many ways to gather evidence and many sources.
Here I shout out to anyone who could conduct case reports – where the experience of a few patients is written up as a paper. This can be the starting point for saying ‘this is something interesting and worth looking at further’.
From there we might be able to generate interest to do a cohort study, possibly supported by a maternity unit, where some parameters are set e.g. specify type of women included i.e. low risk pregnancies, with a baby which is known to be malpositioned (back-to-back etc.) or perhaps exhibiting some signs which may be due to a malpositioned baby such as contractions which slow down or stall or contractions with no progress. Then use the fetal positioning techniques with those women and record what happens.
It may be unrealistic to expect to generate direct evidence of the impact of fetal positioning techniques on labour outcomes, due to the number of compounding factors. However we would hope such studies could support a trend towards improved outcomes.
The way to start may be to find an interested midwife unit – one where ‘natural’ birth is actively promoted. Are there any head midwives reading this who are supportive of these ideas? If so, please do make yourselves known to me!
Thank you to a lovely friend of mine experienced in the world of trials and use of their data (you know who you are!) and also to Jackie, founder of Cherished Births, for this suggestion.
I mentioned this in my previous blog post – this is such a complex and dynamic issue. Any advice or guidance you clued up people out there (researchers, midwives, obstetricians, gynaecologists, scientists, anyone in the know!) can offer on any of these questions would be very welcome. All comments which have come my way so far have been valuable and I would like to thank all of you who have been in touch!
I also say this every blog post, but if I can use fetal positioning techniques myself for both my births with such impressive results (see my first blog post MakeBirthEasierCampaignUK dated 11 May 2015), imagine what trained midwives could achieve using them every day. Women in this country would have a better chance of an easier, uncomplicated, intervention free birth if midwives and other health care providers had training in fetal positioning techniques. To reach that goal, we need evidence and support.
This is a huge opportunity to invest in a more positive future for maternal care in the UK. I am hopeful that I have your support.
For health professionals and others interested in being part of this opportunity, please leave comments / advice / guidance / offers of funding / offers of research team & research facility (!!) on this blog page.
You can contact me via my page at https://www.facebook.com/MakeBirthEasier (particularly if you would like to message me privately)
The Campaign is also on Twitter @MakeBirthEasier, #MakeBirthEasierCampaignUK
Blog written by Alix Fernando
The content of this blog is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.
Make Birth Easier Campaign UK – Research is Needed

‘Women in this country would have a better chance of an easier, uncomplicated, intervention free birth if midwives and other health care providers had training in fetal navigation techniques. To reach that goal, we need evidence.’
Campaign Update
The MakeBirthEasierCampaignUK was launched a week ago and I’m pleased to say it has generated a fair amount of interest and support. I have received some great comments from midwives; “Really great campaign”, “Wonderful work you are doing”, and “I love Spinning Babies and send a lot of women to their website. Great publicity!” Midwives seem to be behind what the Campaign aims to achieve which is for fetal navigation techniques, such as those on SpinningBabies.com, to included in the standard training curriculum for all midwives for use as part of routine care.
The first instalment of this blog (if you haven’t read it yet, click here) has been viewed by over 1000 people in the first week, and the Facebook page Make Birth Easier was visited by 2500 people on the first day! Incredible! The number of views is now well over 5000! I’m over the moon – keep on sharing!
So one week in, what is the next step? My plan is progressing…
Step 1: Generate interest and support from mums and the midwife community. This bit seems to be underway and word is spreading steadily.
Step 2: Generate interest and support from the research community. I have started to receive messages from researchers interested in this opportunity which is fantastic!
We Need Research – I Have Questions!
Maternity care, rather than being based in belief, is best when it is evidence based. For the NHS to go as far as include fetal positioning techniques in routine care, there needs to be clinical research. The Royal College of Midwives (RCM) guidelines on malpositions at the onset of labour state that more research studies are needed to examine the efficacy of midwifery developed skills in diagnosing (malpositions) and non-technological approaches to improving outcomes.
I had a blur of questions flooding into my head; What clinical trials are needed? How would trials be conducted? Which exercises should be included? How could the effectiveness of the exercises be clearly ‘proven’ instead of saying ‘this labour could have progressed in this way naturally’? Birthing mothers are needed who are willing to be part of the trials so how would that be managed? To be significant enough, how far reaching would the trials need to be in terms of areas of the country/numbers of births included? Every labour is different so it cannot be known in advance which techniques will/can be tested, how can this be managed? Am I asking the right questions? What have I missed?!
This is such a complex and dynamic issue. Any advice or guidance you clued up people out there (researchers, midwives, obstetricians, gynaecologists, scientists, anyone in the know!) can offer on any of these questions would be very welcome.
Possible Methodologies
I came up with some ideas and potential answers. The following is for thought/discussion and by no means definitive or a clear plan. Please bear in mind that I am not a medical professional or a researcher.
There is a lot to think about and it would be appropriate to utilise mixed methods to ensure women’s views were taken into account. Given that every labour is different – so it cannot be known in advance which techniques will/can be tested – trying to prove individual techniques may be difficult. Maybe some small pilot studies could be done to look at exercises on this level.
It may be more effective to train midwives throughout a whole birth centre or maternity department with fetal positioning techniques and then compare overall before and after figures for the department. Key target figures such as number of planned csections/emergency csections/number of inductions/epidurals administered/pain relief administered/length of labour etc.
I believe the percentage of births which include medical intervention would reduce and the time in labour would also reduce by using fetal positioning techniques. In this way efficacy would be shown and safety of the techniques.
The study could take place over a defined time period (say for example 6 months) rather than focusing on individual births, while of course still recording the instances where particular techniques were used.
A research team would be required and this team would take on most of the paperwork. Any additional paperwork or notes for completion by the midwives should be simple and kept to a minimum so as not to add to their workload.
There would need to be some form of a control. Potentially, comparison of figures could be done from one department conducting the study against another also taking part, and another not taking part.
Planned csections could be included, as the number of breech/transverse babies requiring planned csection should reduce by using Spinning Babies techniques to turn the baby in advance of labour/planned csection date. This leads on to possible studies including for the use of fetal positioning techniques during late pregnancy during midwife appointments and how this affects the labour. Possibly figures for the number of instances of ECV could also be included. The possibilities are many.
As for reduction in after care, the potential is huge and the money saved by the NHS, well I wouldn’t know where to start. If before and after statistics over a defined period could be gathered for after care required for post natal complications, including post operative infection, special baby care or even post natal depression, this could highlight further areas where fetal positioning could have a direct and positive impact.
Ethics Review
With regard to ‘recruiting’ willing participant birthing mothers for the trials, I am unsure of the protocols. I do know that an ethics review is required. Keeping women and their babies safe and fairly treated is paramount. Women put trust in their care providers and if a midwife were to say ‘I know of an exercise which may help your baby come down more easily/turn to a better position for birth’ I can imagine most women who are able to move freely saying ‘ok let’s try it’. I would!
Midwives Under Pressure
It is important to make this process as easy as possible for midwives so it is welcomed by most and readily accepted by the more sceptical. By making it simple for midwives to incorporate it would assist them in carrying out the new techniques and minimise extra documentation on top of an already heavy workload. For the purposes of the studies/trials, it may be possible that training the midwives in fetal positioning techniques could come under Continued Professional Development (CPD) so it would form part of run of the mill training. Eventually, if the efficacy of fetal positioning for better outcomes is proven (which I wholeheartedly believe it will be), training for existing midwives could possibly be undertaken in a similar fashion i.e. as CPD.
With examples such as Imperial Trust now in the process of expanding its birth centre and creating a proper home birth team, and Watford General Hospital refurbishing the Alexandra Birth Centre, it appears the NHS is leaning towards intervention free birthing in the hope of lowering induction and csection rates. I believe the use of fetal positioning techniques could contribute positively and dramatically to these figures.
Where to Start
I appreciate, despite many years of effective use, that without clinical evidence that any of the Spinning Babies techniques actually do anything, or are safe, it may be difficult to obtain approval for a whole department to use them. Testimonials are not enough. The evidence has to come from somewhere though, and if just one department / research facility / hospital could start this process off and gather some data, this could get the ball rolling for larger, more significant trials. How significant would a study need to be for NICE to get involved?
A key issue for starting any clinical trials is funding. This could come through private investment, sponsorship or potentially the NHS. How loudly will I have to shout to get attention from people with the means to get things done?
Please let me know if I am way off the mark with any of this! As mentioned, I am not from a medical or research background. This instalment of my blog is intended as a basis for discussion and calls for input from health professionals and anyone who can contribute.
If I can use fetal positioning techniques myself for both my births with such impressive results (see my first blog post MakeBirthEasierCampaignUK dated 11 May 2015), imagine what trained midwives could achieve using them every day. Women in this country would have a better chance of an easier, uncomplicated, intervention free birth if midwives and other health care providers had training in fetal positioning techniques. To reach that goal, we need evidence.
This is a huge opportunity to invest in a more positive future for maternal care in the UK. I am hopeful that I have your support.
For health professionals and others interested in being part of this opportunity, please leave comments / advice / guidance / offers of funding / offers of research team & research facility (!!) on this blog page.
You can also contact me via my page at https://www.facebook.com/MakeBirthEasier (particularly if you would like to message me privately)
The Campaign is also on Twitter @MakeBirthEasier, #MakeBirthEasierCampaignUK
Blog written by Alix Fernando
The content of this blog is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.
Make Birth Easier Campaign UK

An excerpt of this article was published in
The National Childbirth Trust (NCT) magazine in June 2015.
‘I turned my back-to-back baby and regulated my own contractions to avoid induction and cesarean section – most British midwives don’t know how to do what I did – #MakeBirthEasierCampaignUK aims to change that.’
Mum-To-Be Voyage of Medical Discovery
As an expectant first time mum I, like many other first-time mums-to-be, spent a lot of time doing research into all things related to pregnancy, labour and babies. Firstly I found an article on hypnobirthing in the newspaper. Then through my hypnobirthing teacher, it was in the last few weeks of my pregnancy that I discovered the website SpinningBabies.com which extends the concepts of optimal fetal positioning through non-invasive maternal postures and positioning during pregnancy and labour. Like a lot of expectant mums, I was hoping for a vaginal birth without medical intervention and the suggestion that simply through exercises and positional techniques, I could potentially find solutions for a range of possible complications in labour was fascinating.
Spinning Babies is a project by Gail Tulley, an American midwife. The website teaches exercises and positional techniques for helping to prevent fetal malposition or malpresentation in pregnancy or, for use during labour, if there is no progress or contractions are erratic, slow down or stop. Even reducing back or hip pain in labour. Techniques can encourage the rotation of transverse, breech and back-to-back babies and can even help the baby to engage.
A labour which is slow to progress, or contractions that slow down or stall can commonly be signs of a malpositioned or malpresented baby. While breech and back-to-back (medically known as Occiput Posterior or OP) are the most well known malpresentation and malposition respectively, there are all sorts of funny or awkward positions babies can get into in the womb. Often, if you can create a little bit more space for your baby to move by balancing the uterus and balancing/releasing the pelvic floor muscles / ligaments, your baby may be able to manoeuvre to align the smallest part of its head correctly with your pelvis/cervix and your labour may progress more smoothly and without delays. Gail Tulley has used and taught this range of techniques for many years, many of which come from chiropractic techniques.
The more I read on the Spinning Babies website, the more I was amazed. Something as simple as the baby’s head being tilted to the side slightly (asynclitism), or its chin not tucked to its chest (flexion), can add several hours and much effort to a labour. Very long labours can lead to mum or baby becoming tired or distressed which can often result in intervention, assisted delivery or caesarean section. This range of techniques can resolve many of these issues, so I decided to study the techniques section of the website in depth and used several exercises with, in my opinion, dramatic effect on both my labours.
My Incredible Births
My first baby struggled to engage in my pelvis for weeks without success, moving back up within 12-24 hours of engaging. I looked at exercises on SpinningBabies.com, in particular the ‘Side Lying Release’ (or ‘Pelvic Floor Release’), which relaxes and balances pelvic floor muscles and ligaments. I had a very strong pelvic floor from years of exercise and it’s probable that a lot of time spent slouching at desks, driving, carrying a bag on one shoulder, and crossing my legs had created imbalances in my uterus which, combined with my strong pelvic floor muscles, had reduced space in my pelvis and was hindering my daughter’s progress even before labour had started!
My first labour began with regular but weak, short contractions and no progress. My contractions were not getting longer, stronger or more frequent. I asked my husband to help me with some Spinning Babies exercises. We performed the ‘Rebozo’ exercise followed by the ‘Side Lying Release’. I was glad to have practiced this second one during the week before labour as it can be a little disconcerting and awkward on the first try! I have since discovered that if the instructions are not followed exactly, for the ‘Side Lying Release’ in particular, the exercise doesn’t have much effect so I am very glad I paid such attention to the detailed instructions on the website! Within a couple of contractions after completing the ‘Side Lying Release’ my stagnant labour transformed into full active flow. Instead of having a long, slow and tiring labour, suddenly I was in established labour with very strong, efficient surges, close together and lasting over 60 seconds. Exactly what I had hoped for! I went on to hypnobirth my little girl at my nearest Birthing Centre in the birth pool, without any drugs or intervention of any kind.
My second labour was very different. I had stop-start contractions for a week or so. They started every time I marched up nearby hills and, erratic as they were, they stopped during the evening or overnight. I guessed this was because my little boy was back-to-back in the final two weeks of pregnancy after months of being well positioned. I had planned a homebirth as statistically second births at home are at least as safe as the hospital and have less intervention, but I was still uneasy about the prospect of a home birth with a back-to-back baby. At 40 weeks +12 days, having an induction booked for 7am, I was nevertheless determined I wasn’t going to give in to a medicated start to labour without doing everything I could to avoid it. Introducing any one intervention can often lead to more interventions (this is known as the cascade of interventions) and I wanted a medically unassisted vaginal birth. So at 11pm the night before induction was due, I went out stomping up and down hills again at such speed that my husband had to ‘keep up’!
At 4am the next morning – induction day – I hadn’t yet given up hope of an intervention free birth and began marching on the spot in our bedroom which started contractions again albeit very erratic at seven minutes, then twelve, five, ten and so on. On-going irregularity in length, strength and frequency of contractions can be an indication that the baby may be in a less than optimal position for birth…it was time for Spinning Babies!
I chose the ‘Abdominal Lift and Tuck’ technique as this is a favoured method for turning a back-to-back baby and also useful for any baby that is not engaged in the pelvis at the start of labour. As the ‘Abdominal Lift and Tuck’ was something I could do alone, I left my husband sleeping soundly. Over the course of ten contractions I followed the website instructions to the letter, which took just over an hour. By the end of the ten contractions they were finally settling into a regular pattern as my baby had turned into a better position. With huge relief and only half an hour to spare, I made the call at 6.30am to cancel my induction appointment! Later that day I gave birth to my son in the birthing pool in my living room, again using hypnobirthing and without any drugs or intervention of any kind.
For me, the combination of hypnobirthing (to help my relaxation and comfort level mentally and physically), with Spinning Babies exercises (for aligning my babies correctly with my pelvis and smoothing their route into the world), was invaluable to prepare for easier, intervention-free births.
Empowering Mothers
Spinning Babies techniques helped a friend to turn her second breech baby to head down so she was able to have a VBAC (vaginal birth after caesarean) and also helped my sister have a smooth birth with her second child. My sister’s first labour had been long and painful and proved quite traumatic due to the very difficult position of her baby. To avoid this second time around, in late pregnancy, she prepared for labour using the ‘Rebozo’, the ‘Forward Leaning Inversion’ and the ‘Side Lying Release’ techniques. Our mum was with my sister during labour, and having studied some of the Spinning Babies techniques with me, was ready to assist her into helpful positions.
Another friend had to be induced at 37 weeks due to very high blood pressure. Her baby was transverse at the time and so she asked her obstetrician if it was safe to wait for a few hours more and try some Fetal Navigation Techniques. They were happy to wait and sure enough baby turned head down. They induced immediately and within only two hours her baby was born smoothly! She was amazed that she was up and walsking around on the same day feeling ok because her two previous babies, also with early induction, were long and difficult forceps births which affected her recovery and comfort. She wished she had known about the techniques before baby number one!
As many of the techniques can be performed by women and their partners themselves, it can be very empowering for women and allow them to feel in control and have ownership of their own birthing experience. This was precisely how I felt from the moment I started reading SpinningBabies.com. I felt I had a toolkit from which I could draw out tools to change the course of my labour if it wasn’t progressing as planned. It was liberating to know I could take control and this is exactly what I did!
I believe every pregnant woman should have access to these Fetal Navigation Techniques and therefore stand a better chance at experiencing an uncomplicated, intervention-free birth. I am impassioned to do something about this. After all, if I can do what I did with SpinningBabies.com exercises, imagine what midwives could achieve with them every day. I asked myself the question – why don’t midwives in the UK use these techniques?
For Midwives and Care Providers
In my discussions with midwives and mums-to-be, I have found that very few people in this country have even heard of SpinningBabies.com, although there are some UK midwives and doulas who are already transforming their practices (unofficially) with the techniques. I heard a report of midwives who tried a ‘Side Lying Release’ on their mum-to-be while she was being prepared for an emergency caesarean section (due to long labour) in the North-West of England. The surgery was cancelled just in time as the baby arrived within minutes of the technique being used! Just one other example of the amazing results which can be achieved!
I would dearly love to see Fetal Navigation Techniques officially adopted by midwives, antenatal teachers and doulas but, as is absolutely right, the British NHS (National Health Service) require evidence based clinical trials to prove they are safe and effective. Without any evidence at all, many healthcare organisations would not likely give serious consideration to doing their own clinical research. So the road to having large clinical studies even being considered is potentially a long and arduous one and this is a stumbling block to bringing these techniques into mainstream use by UK care providers.
However, this is a clinical issue and doesn’t stop women (and their partners) using the exercises for themselves. Many of the techniques are so simple and easy to perform for women with low risk pregnancies. There is clear safety advice for each technique on the Spinning Babies website which should always be referred to before attempting any of the exercises and, discussing the exercises with your midwife or obstetrician is recommended as they can advise on suitability for individual pregnancies.
Supporting the National Health Service
The British NHS is hugely short of funding, and midwives are short staffed and stretched to their limits under tremendous pressure. I believe that using these techniques the NHS could naturally help to reduce the time each woman is in labour which would give midwives more precious time with each birthing mother. The techniques can facilitate easier, faster and safer vaginal birthing thus reducing the ever increasing number of caesarean sections performed and the amount of drugs administered. It could also reduce the necessity for after-care for mums and babies – cutting down on post operative infections reducing traumatic births and even helping to reduce the occurrence of post natal depression. Speaking from a business perspective, collectively these reductions could save a huge amount of money for the NHS and help ease pressure on midwives in so many ways. More importantly this would save a lot of pain and trauma for women and babies!
The Campaign for Positive Change
I have launched a media campaign – Make Birth Easier Campaign UK – to raise awareness of Fetal Navigation Techniques (aka Spinning Babies) in the UK to a level where midwives and obstetricians want to learn about them and mums-to-be are fully informed and can request use of these techniques in their birth plans. I am hopeful that with key medical professionals on board with the theory, I can push for clinical research for these techniques and move closer to the goal of Make Birth Easier Campaign UK – Fetal Navigation Techniques being part of standard maternity care provider training curriculums and used routinely in mainstream maternity care; labour wards, birthing centres, and home birthing teams.
Clinical Evidence is Required
We know they work and there are no reports of safety issues when using the techniques as directed. However, having great stories about how well and how quickly Fetal Navigation Techniques work is not enough – it is not evidence. Official clinical studies are required to prove these techniques. Once there is some clinical evidence of those two basic and fundamental questions; do they really work, and, are they safe; then larger clinical research studies are sure to follow and eventually the evidence level will be hard to ignore and the techniques will be incorporated into maternity training (that’s the plan!). All it will take to start the ball rolling is one person, with the facility and funding to run a clinical study, to notice this campaign and get involved. I am determined to give women in this country a better chance at the birth they want and deserve. It seems so simple, and yet getting there is so complex!
Follow the Campaign
An excerpt of this article was published in The National Childbirth Trust (NCT) magazine in June 2015.
You can follow the progress of Make Birth Easier Campaign UK here at this website and on:
Twitter @makebirtheasier
#MakeBirthEasierCampaignUK
#SpinningBabies
and
https://www.facebook.com/MakeBirthEasier
Written by Alix Fernando
Spinning Babies is on Facebook and Gail Tulley can be found on Twitter @SpinningBabiesLady.
Also on Facebook is the UK group – ‘Unlocking Birth: techniques to resolve and prevent malposition’.
The content of this website is not intended, and should not be read as constituting medical advice, diagnosis or treatment. Always consult your doctor, midwife or other qualified healthcare provider before making any changes to your birth plan or recommended routine.

{kind=link}